Clear Sky Science · en
Noninvasive biventricular pressure-strain-volume loop-derived myocardial work analysis in competitive athletes
How hard does an athlete’s heart really work?
Competitive athletes push their bodies to extremes, and nowhere is that more evident than in the heart. Yet, standard heart tests at rest can make even a well-trained heart look only “average” or even slightly weak. This study introduces a new, more revealing way to measure how powerfully both sides of the heart pump in athletes—without putting a catheter into the heart—helping doctors distinguish between healthy sports-related changes and early signs of disease.
Looking beyond routine heart checkups
For decades, doctors have known that regular intense training enlarges the heart’s chambers, thickens its walls, and lowers the resting heart rate. These changes, often called the “athlete’s heart,” allow for a big surge in blood flow during exercise. But the most common measures of heart function—such as ejection fraction (how much blood is pumped out with each beat) and strain (how much the heart muscle shortens)—are strongly influenced by blood pressure and how full the heart is. Because athletes’ hearts are bigger and often less filled at rest, these standard readings can look deceptively low, even when the heart muscle is actually stronger than average.
A 3D movie of the heart at work
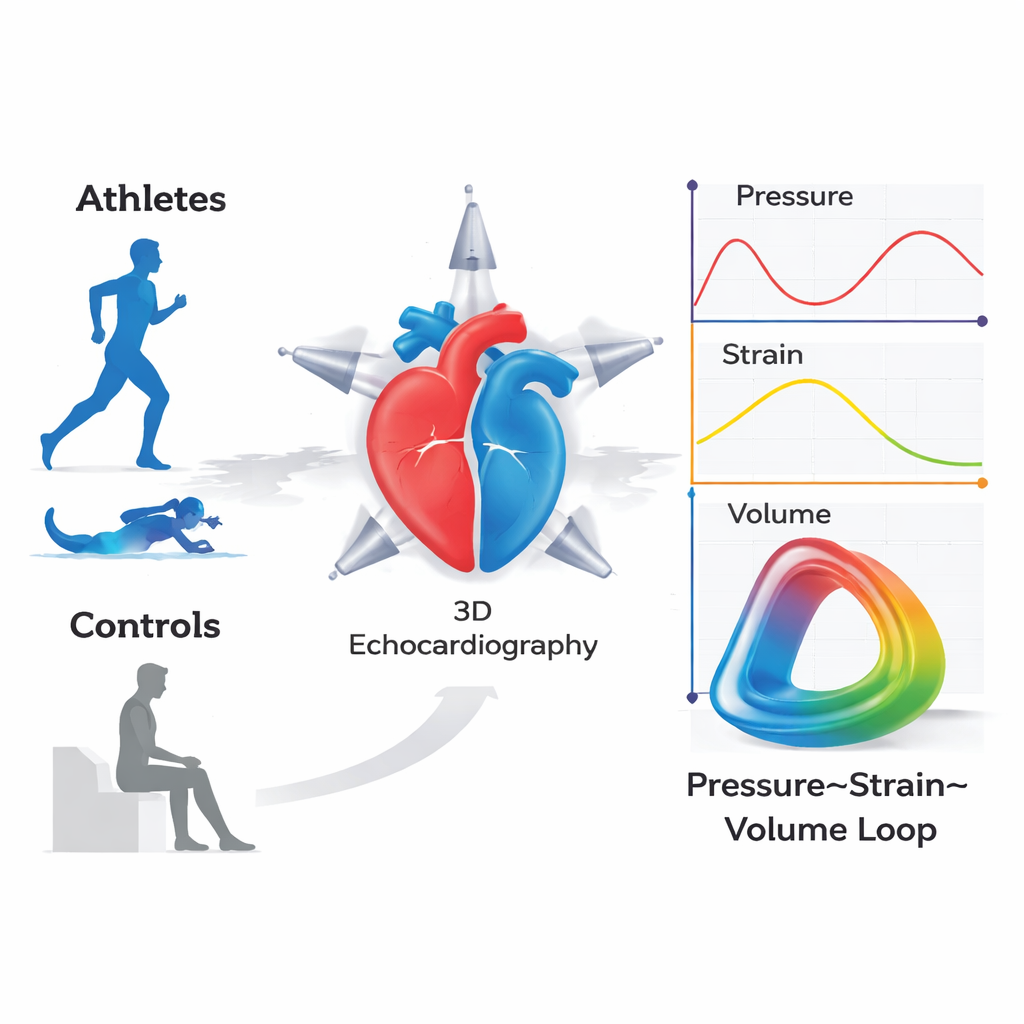
The researchers set out to build a more realistic picture of how an athlete’s heart works by combining three pieces of information: blood pressure, how the heart muscle deforms, and how the heart’s chambers change in size with each beat. Using three-dimensional echocardiography (a 3D heart ultrasound), they recorded how the left and right ventricles filled and emptied in 260 competitive athletes and 24 healthy but sedentary adults. At the same time, they estimated pressure inside the heart from arm blood pressure and from a jet of blood leaking backward through a right-sided valve, and tracked how much the heart muscle stretched and shortened with each heartbeat.
By merging these three signals, the team created what they call pressure–strain–volume loops—essentially a 3D movie frame of how hard the heart muscle works at each instant. From these loops, they calculated new “volume-adjusted myocardial work” numbers, which represent how much useful work the left and right ventricles perform, scaled to the size and filling of the pumping chamber. This makes the measurements far less dependent on changing loading conditions, such as how much blood returns to the heart or the blood pressure at the time of the exam.
What makes an athlete’s heart special
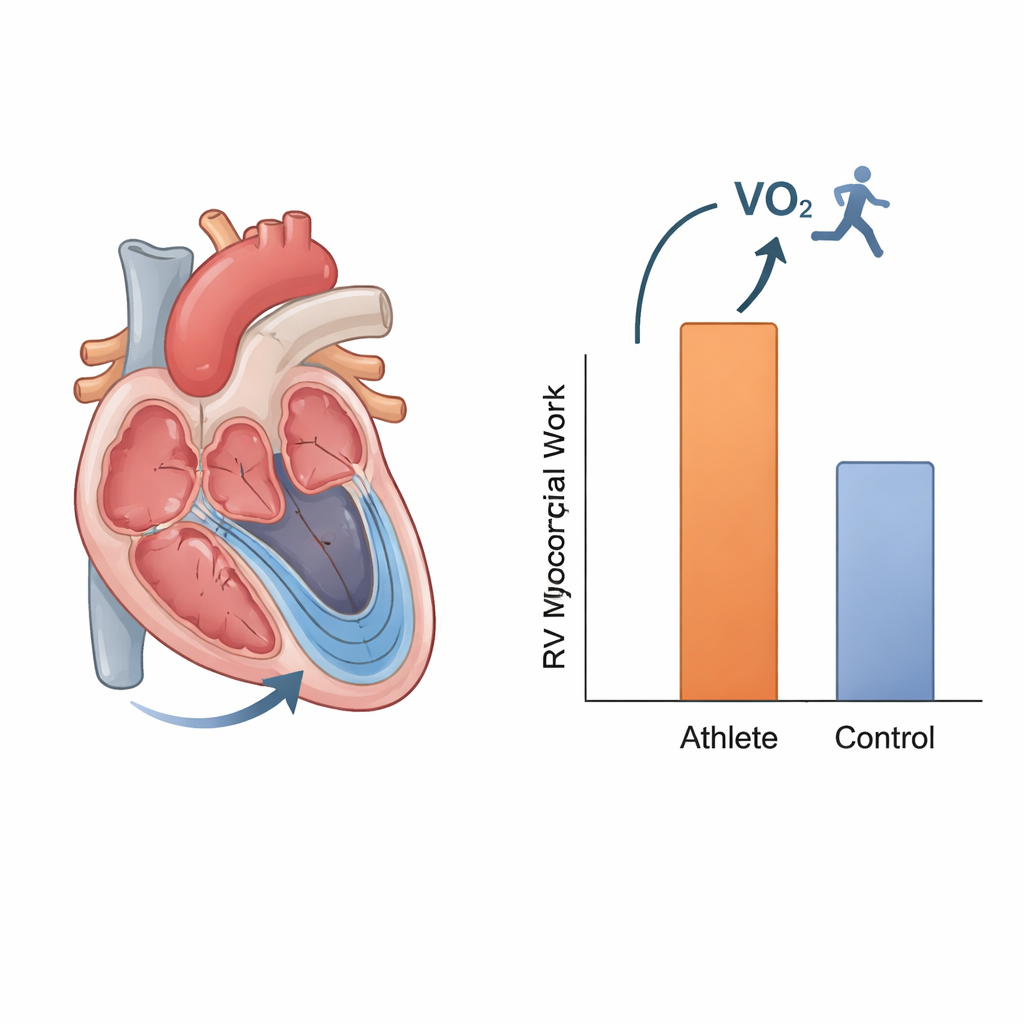
When the team compared athletes with non-athletes, the standard numbers were misleading: athletes had lower resting ejection fractions and slightly lower strain in both ventricles, which might suggest weaker pumping if viewed in isolation. However, their volume-adjusted myocardial work values were clearly higher for both the left and right sides of the heart. In other words, when the bigger chamber size and different filling conditions were taken into account, the athletes’ hearts were doing more effective work with each beat, even while they were just lying on an exam table.
The most striking finding involved the right ventricle, the chamber that pumps blood to the lungs. A specific right-sided index, called volume-adjusted global myocardial work, showed the strongest link to peak exercise capacity—the amount of oxygen athletes could use on a treadmill test—and remained an independent predictor even after accounting for age, sex, body size, heart rate, and sport type. This suggests that how powerfully the right ventricle works at rest is closely tied to how far an athlete can push their performance.
Differences by sex, age, and sport
The study also explored how these new measures vary across different groups of athletes. Men tended to have larger heart chambers and lower conventional measures such as ejection fraction and strain, but higher volume-adjusted work values in both ventricles than women, reflecting their larger, more remodeled hearts. Adult athletes showed higher left-ventricular work indices than adolescents, in line with more years of training, while right-ventricular work changed less with age, hinting that the right side may adapt earlier and then plateau. Endurance athletes—such as distance runners and swimmers—had the highest exercise capacity and showed subtle signs that their right ventricles operate under greater volume load, again underscoring the importance of examining right-sided function carefully.
Why this matters for athletes and their doctors
For athletes, the key message is reassuring: when properly measured, their hearts are not “borderline weak” but often more powerful and efficient, especially on the right side. For sports cardiologists, this new pressure–strain–volume approach offers a noninvasive way to better tell the difference between healthy adaptations to training and early disease in athletes whose standard test results fall into a gray zone. In the future, these refined measures of myocardial work could help guide training, monitor long-term heart health in elite competitors, and flag those rare cases where an apparently “strong” athletic heart is actually under strain for the wrong reasons.
Citation: Ferencz, A., Szijártó, Á., Turschl, T.K. et al. Noninvasive biventricular pressure-strain-volume loop-derived myocardial work analysis in competitive athletes. Sci Rep 16, 4848 (2026). https://doi.org/10.1038/s41598-026-35206-0
Keywords: athlete’s heart, cardiac remodeling, right ventricle, myocardial work, exercise capacity