Clear Sky Science · en
Optimizing butorphanol-dexmedetomidine dosing for managing catheter-related bladder discomfort post-anesthesia: a randomized trial
Why this matters after surgery
Many people wake up from surgery with an unpleasant surprise: a burning, urgent feeling in the lower belly caused by the urinary catheter placed during the operation. This problem, called catheter-related bladder discomfort, can make patients restless, pull at their tubes, and strain fresh surgical wounds. The study summarized here tested whether a specific drug combination could quickly calm this discomfort while keeping breathing safe and avoiding overly deep sedation. Its findings could change how recovery rooms worldwide manage one of the most common sources of distress right after anesthesia.
What is this uncomfortable feeling?
Urinary catheters are thin tubes inserted into the bladder to drain urine during and after many operations. While they are crucial for safety and surgical precision, they often irritate the bladder lining. Patients then feel burning pain above the pubic bone, a strong urge to urinate, or a sense that the bladder is constantly full, even though urine is already draining. Up to nine out of ten patients may notice some level of this discomfort, and nearly half experience it strongly enough to become agitated. That agitation, in turn, can raise blood pressure and heart rate, increase pain, and even put stitches and catheters at risk. Existing drugs to treat this problem may help but often slow wake-up, cloud thinking, or depress breathing, especially in older or fragile patients.
A closer look at three drug options
To find a better balance between comfort and safety, researchers in China ran a randomized trial in adults waking from surgery who had moderate-to-severe catheter discomfort. All had undergone general anesthesia with a urinary catheter. Once in the recovery room, 102 eligible patients were randomly assigned to receive one of three intravenous drug combinations. Every group received the sedative-analgesic dexmedetomidine in the same low dose. One group also received sufentanil, a powerful standard opioid painkiller. A second group received a low dose of butorphanol, and a third group received a higher dose of butorphanol. Butorphanol acts mainly on a different set of pain pathways that are especially important in deep, internal "visceral" pain, such as from the bladder or intestines.
How the researchers measured comfort and safety
Patients were carefully monitored for an hour in the recovery room and then followed longer for pain and overall recovery. The team rated bladder discomfort on a simple 0–3 scale, where 0 meant no symptoms and 3 meant severe pain with agitation or attempts to remove the catheter. They counted a treatment as successful when the score fell to 1 or less. They also tracked blood pressure, heart rate, oxygen levels, breathing rate, pain scores, and how sleepy or alert patients were. Breathing trouble meant slow breathing or low oxygen without extra support, while oversedation meant the patient was more deeply asleep than considered safe for routine recovery.
What the study found about relief and risks
All three drug combinations eased bladder discomfort, but they did not perform equally. Fifteen minutes after treatment, only about one in four patients given dexmedetomidine plus sufentanil reached the target comfort level, compared with more than four in five on the low-dose butorphanol mix and about two in three on the higher-dose butorphanol mix. By an hour, response rates in the butorphanol groups were above 90%, and nearly all patients on the lower dose achieved good relief. The low-dose butorphanol group also had the steadiest heart rate and experienced fewer episodes of slowed breathing than the sufentanil group. Pain scores outside the bladder were generally better with low-dose butorphanol, and patients in this group were less likely to be excessively drowsy soon after treatment than those who received either sufentanil or the higher butorphanol dose.
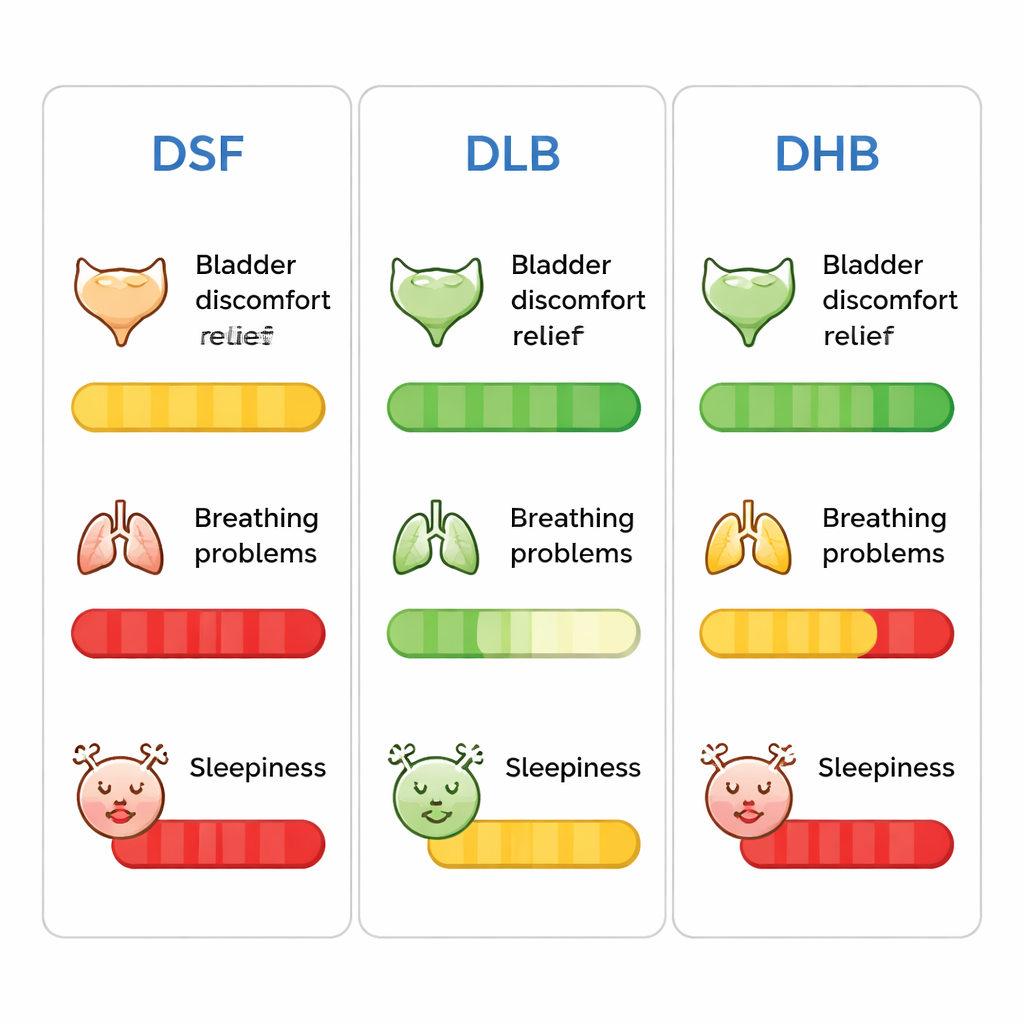
What this means for patients in recovery
Putting the findings together, the study suggests that pairing a small dose of dexmedetomidine with a modest dose of butorphanol provides fast, strong relief of catheter discomfort while limiting risks to breathing and avoiding overly deep sleep. Higher butorphanol doses did not clearly improve bladder relief but did increase early oversedation, and the combination with sufentanil caused more breathing problems and slower recovery of alertness. For patients, this optimized mix could mean waking from surgery with less burning and urgency in the bladder, more stable vital signs, and a clearer head. For hospitals, it offers a practical, evidence-based protocol that could make recovery rooms calmer, safer, and more comfortable for a common but often underappreciated source of distress.
Citation: Wang, YL., Zhang, Y., Wang, QB. et al. Optimizing butorphanol-dexmedetomidine dosing for managing catheter-related bladder discomfort post-anesthesia: a randomized trial. Sci Rep 16, 4788 (2026). https://doi.org/10.1038/s41598-026-35071-x
Keywords: catheter-related bladder discomfort, postoperative recovery, butorphanol, dexmedetomidine, urinary catheter