Clear Sky Science · en
Biomechanical study on different internal fixation methods for treating Mayo type IIA olecranon fractures of the ulna
Why fixing a broken elbow tip matters
Breaks of the bony tip of the elbow, called the olecranon, are common when people fall on an outstretched arm. Surgeons have several ways to hold these fractures together with metal wires or plates so the bone can heal and the elbow can bend normally again. But different methods have different strengths, risks, and costs. This study used laboratory testing on model bones to ask a practical question that affects many patients: how deep should common wires be placed inside the bone, and when is a more expensive plate truly stronger?
Different ways to hold the elbow bone together
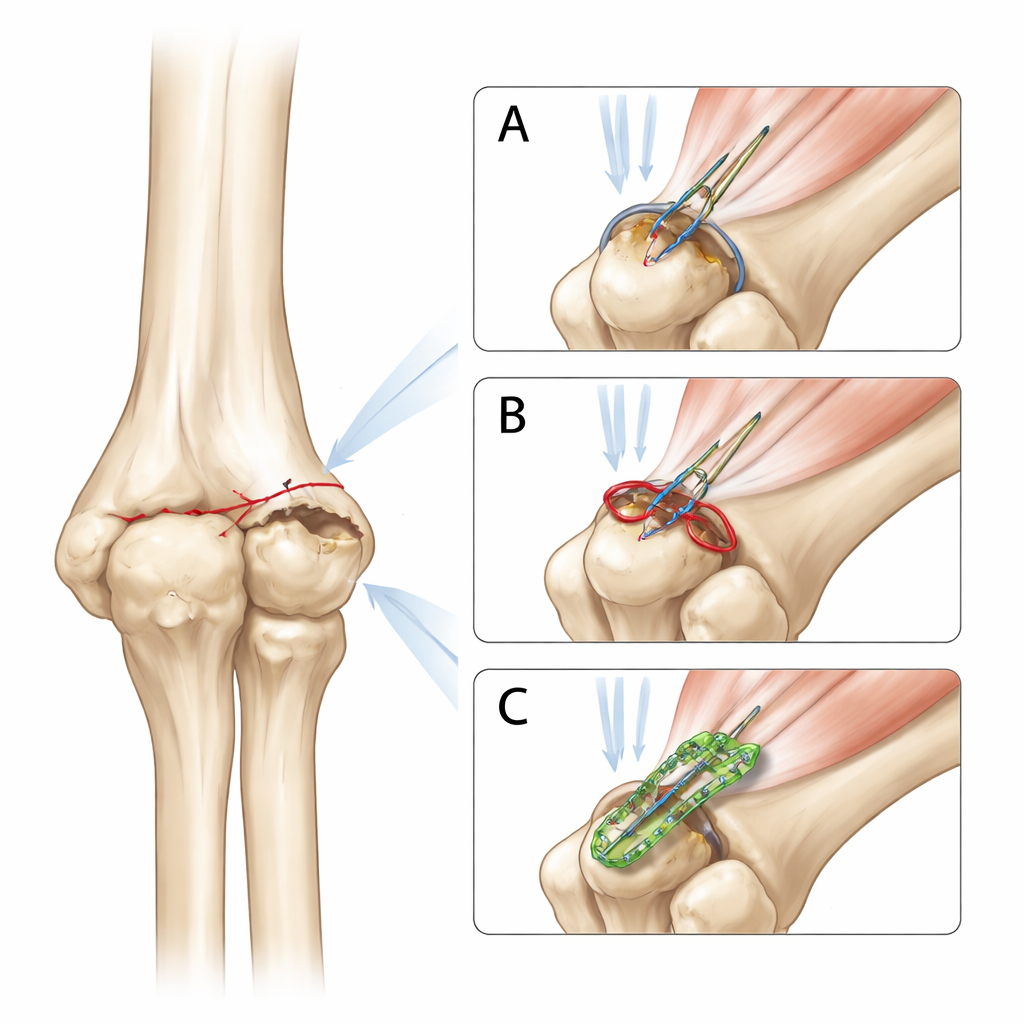
The olecranon is part of the ulna, one of the two forearm bones, and it serves as the anchor for the powerful triceps muscle that straightens the elbow. When this bump breaks in a simple, stable pattern known as a Mayo type IIA fracture, surgeons most often use a “tension band” technique. In it, two thin metal pins (Kirschner wires, or K-wires) and a loop of wire work together to press the fracture surfaces tightly together when the triceps pulls. Alternatives include driving the pins all the way through the front of the bone (bicortical fixation) or using a contoured metal plate screwed onto the back of the ulna. Each approach trades off stability, risk of irritation or nerve injury, and cost.
Building and testing model elbows
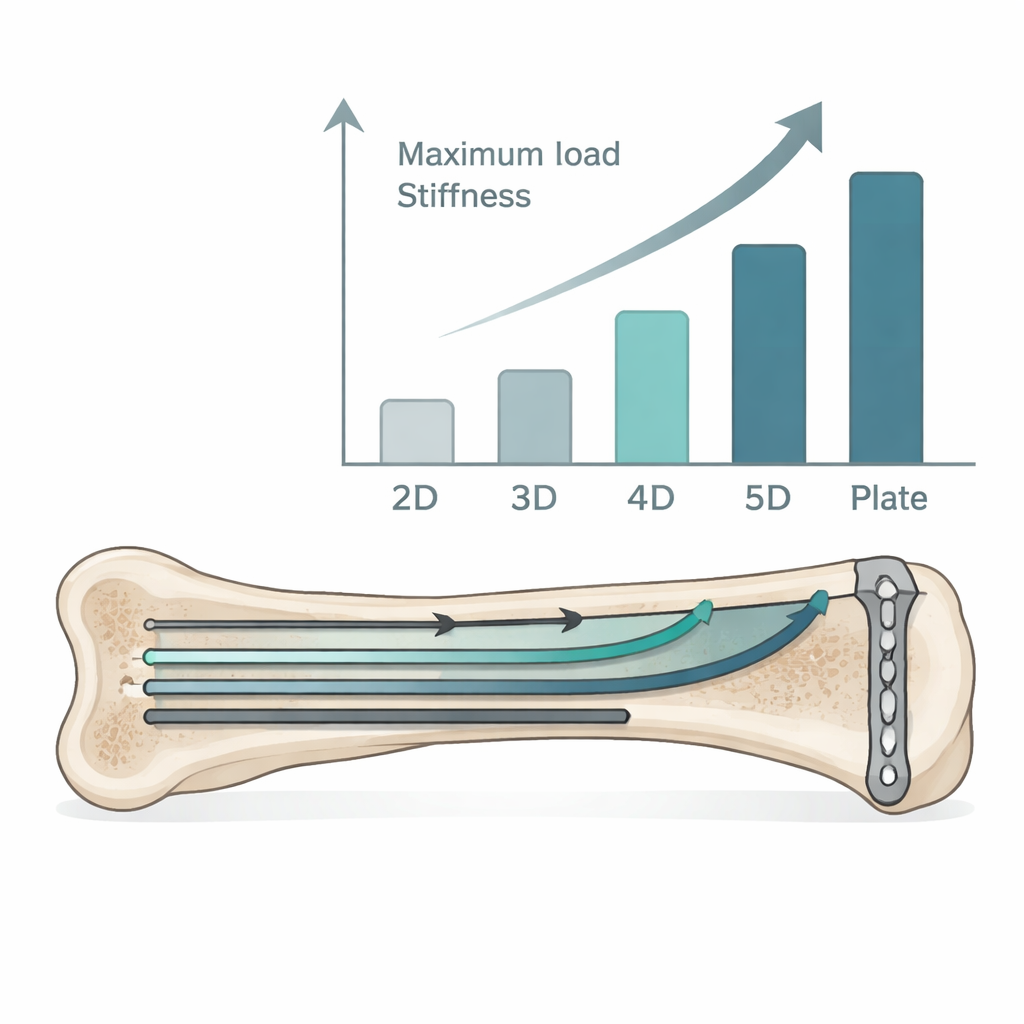
To compare these options in a controlled way, the researchers used eighteen synthetic ulna bones that closely mimic real human bone. They created the same standardized transverse fracture in each model. Then they repaired the break using six different methods, three specimens per group. Four groups received the intramedullary tension-band technique, where two K-wires were placed down the center canal of the bone but stopped at different depths: two, three, four, or five times a measured distance between landmarks on the ulna. A fifth group had conventional bicortical K-wires that pierced the far front surface of the bone, and the sixth group had a locking plate fixed with screws along the back of the ulna.
How strong were the repairs under pull from the triceps?
Each repaired bone was mounted in a mechanical testing machine that mimicked a bent elbow at 90 degrees. A metal cable pulled on the olecranon tip to imitate the triceps muscle trying to straighten the arm. The machine slowly increased the pull while measuring how much the fracture gap moved. From these measurements, the team calculated two key properties: maximum load, meaning how much force the repair could withstand, and stiffness, meaning how rigidly it held the bone pieces together. Testing stopped once the fracture had shifted by 2 millimeters, a small but meaningful movement.
Deeper wires made a clear difference
The results showed a clear pattern. As the K-wires in the intramedullary tension-band groups were placed deeper inside the bone, both maximum load and stiffness steadily increased. The shallowest placement (two times the reference depth) was the weakest. When the wires reached four times that depth, the construct became stronger and stiffer than the standard bicortical K-wire method, even though the bicortical pins pass through both sides of the bone. Going to five times the depth improved strength slightly more. However, the locking plate construct still outperformed all wire-based methods, providing the highest resistance to pulling forces and the greatest stiffness overall.
What this means for patients and surgeons
For patients with a simple, stable olecranon fracture, these findings suggest that surgeons can boost the strength of a familiar, relatively inexpensive wire technique simply by placing the pins deep enough inside the bone canal—about four times a standard anatomical distance. At that depth, the repair is at least as strong as, and in this study stronger than, the more traditional method of driving pins through the far side of the bone, which carries more risk of irritating nerves and limiting rotation. While plates remain the strongest option in the lab, careful use of intramedullary K-wires may offer a practical balance of safety, stability, and cost in many everyday elbow fracture cases.
Citation: Zhang, J., Fang, Y., Zhuang, Y. et al. Biomechanical study on different internal fixation methods for treating Mayo type IIA olecranon fractures of the ulna. Sci Rep 16, 4947 (2026). https://doi.org/10.1038/s41598-026-35057-9
Keywords: olecranon fracture, tension band wiring, Kirschner wire, locking plate fixation, elbow biomechanics