Clear Sky Science · en
The red cell distribution width to albumin ratio as a novel predictor of 180-day mortality in lung cancer patients
Why this matters for people with lung cancer
Many people with advanced lung cancer eventually become critically ill and require care in an intensive care unit (ICU). Families and doctors then face agonizing questions: who is likely to survive the next few months, and who might benefit from more aggressive treatment versus a focus on comfort? This study explores whether a simple number, calculated from two common blood tests, can help predict the chances of surviving the next six to twelve months.
A simple ratio from routine blood tests
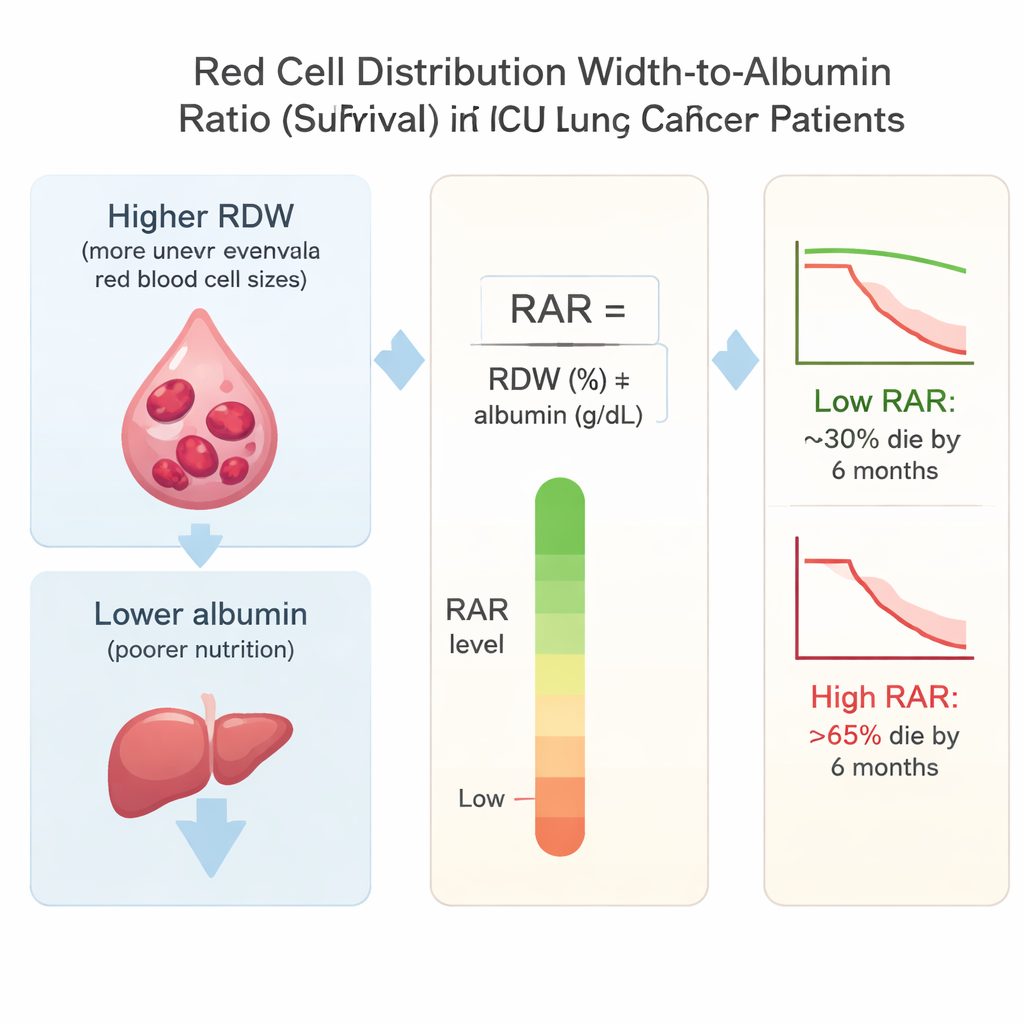
The researchers focused on the red cell distribution width-to-albumin ratio, or RAR. Red cell distribution width (RDW) reflects how uneven in size a person’s red blood cells are, which tends to increase with long-lasting inflammation and illness. Albumin is a protein made by the liver; low levels often signal poor nutrition and severe disease. By dividing RDW by albumin, RAR combines information about both inflammation and nutritional health—two key factors that drive decline in lung cancer.
Who was studied in the ICU
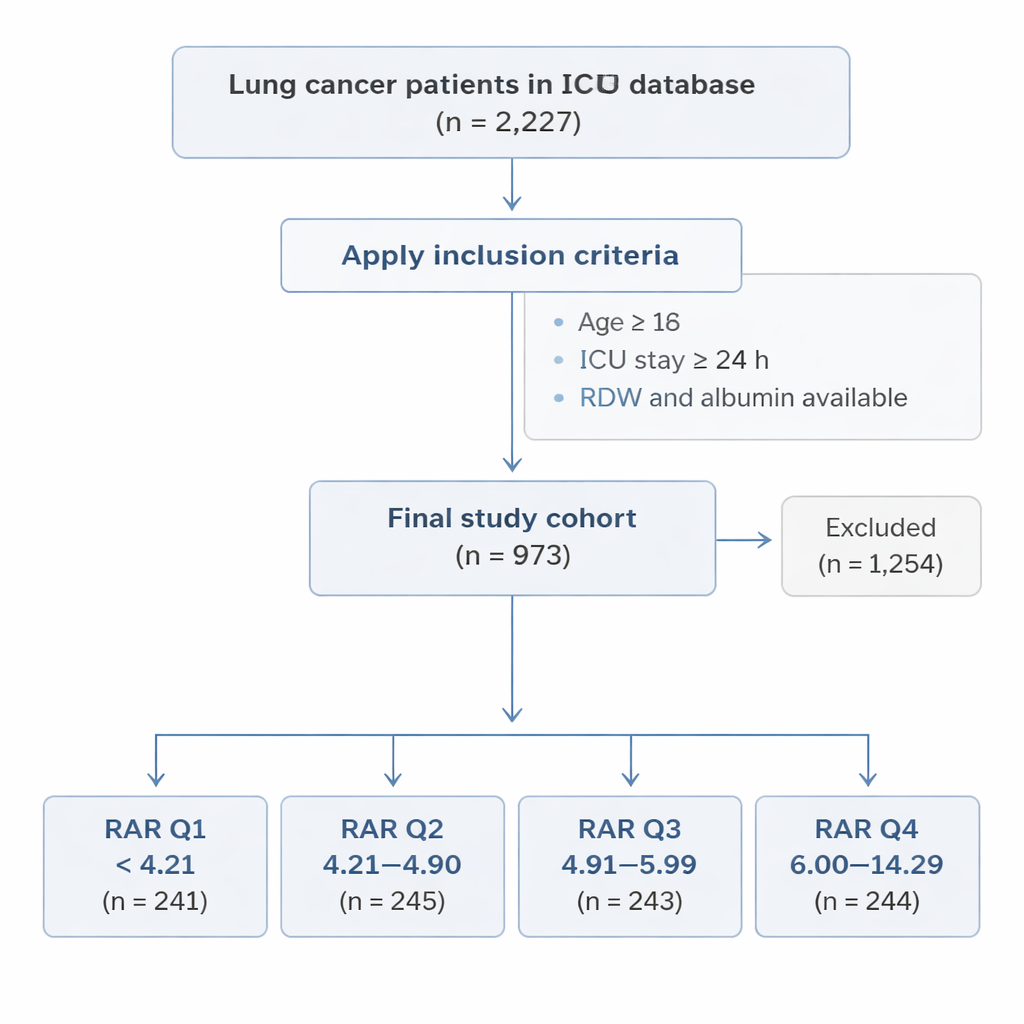
Using the large MIMIC-IV hospital database from Boston, the team identified 973 adults with lung cancer during their first ICU stay. All had been in the ICU for at least 24 hours and had both RDW and albumin measured within the first day. Patients were divided into four groups based on their RAR value, from lowest (Q1) to highest (Q4). The researchers then followed what happened to each person over the next 180 days (about six months) and 365 days (one year), looking at whether they survived or died from any cause.
Higher ratio, higher risk
The pattern was striking. Patients in the highest RAR group had far worse outcomes than those in the lowest group. About 31% of patients in the lowest group died within 180 days, compared with more than 66% in the highest group. At one year, deaths rose from roughly 43% in the lowest group to over 73% in the highest. Even after the researchers adjusted for age, vital signs, other illnesses, and how sick the patients looked by standard ICU scores, each step up in RAR was linked to a higher risk of death. In the highest group, the risk of dying within six months was more than doubled compared with the lowest group.
How this compares with existing ICU scores
Doctors in ICUs commonly use tools like the SOFA score to estimate how likely a patient is to survive, but these scores focus on short-term organ failure rather than the long-term impact of cancer, inflammation, and wasting. When the team compared RAR with SOFA, the ratio did a better job of distinguishing who would be alive at six and twelve months. RAR’s accuracy was modest—it did not “perfectly” sort survivors from non-survivors—but it clearly outperformed SOFA alone. Notably, RAR worked best in patients who were not yet in the very highest category of organ failure, suggesting it is especially useful as an early warning sign rather than a late-stage measure.
What this could mean for patients and families
For families and clinicians facing critical decisions, RAR offers a low-cost, easy-to-calculate marker that uses tests already drawn in almost every ICU. A high RAR soon after admission signals that a lung cancer patient has a substantially higher chance of dying within the next six to twelve months, even if they do not yet appear to be in complete organ failure. This information could help guide conversations about goals of care, prompt closer monitoring, and encourage timely efforts to improve nutrition and control inflammation. While the ratio is not perfect and needs to be confirmed in future studies, it shows promise as a practical tool to help navigate some of the hardest decisions in advanced lung cancer.
Citation: Zhang, L., Liu, T., Wang, G. et al. The red cell distribution width to albumin ratio as a novel predictor of 180-day mortality in lung cancer patients. Sci Rep 16, 4773 (2026). https://doi.org/10.1038/s41598-026-35005-7
Keywords: lung cancer, intensive care, blood test biomarkers, nutrition and inflammation, mortality risk