Clear Sky Science · en
Modelling lung and muscle oxygen diffusion capacities from sea-level to Mount Everest
Why breathing at extreme heights matters
Imagine sprinting up a steep hill while the air gets thinner with every step. Mountain climbers, endurance athletes, and even people with heart or lung disease all face a version of this challenge: how well can their bodies move oxygen from the air into working muscles when oxygen is scarce? This study uses a mathematical model, fed with a century of high‑altitude expedition data, to explore how efficiently our lungs and muscles can absorb oxygen from sea level all the way up to the summit of Mount Everest.
Following oxygen from air to muscle
To understand performance at altitude, scientists track an "oxygen cascade"—the step‑by‑step journey of oxygen from inhaled air, through the lungs and bloodstream, and finally into muscle cells where it fuels energy production. Two critical but hard‑to‑measure steps are how easily oxygen diffuses across the lung’s air–blood barrier (lung diffusion capacity) and from tiny blood vessels into muscle fibers (muscle diffusion capacity). Direct measurements at high altitude and during all‑out exercise are rare, so the authors turned to modelling, building on classic physiology equations that balance how much oxygen blood carries and how quickly it can move across tissues.
Building a virtual ascent to Everest
The researchers compiled maximal‑effort exercise data from many studies performed at altitudes ranging from sea level to near the top of Everest, including famous experiments like Operation Everest II. These datasets included oxygen uptake, cardiac output, blood oxygen levels, and hemoglobin concentration. They then used statistical fits to predict how each of these variables changes every 250 meters of altitude gain. With these inputs, a numerical method known as Fibonacci’s method iteratively solved mass‑balance equations along lung and muscle capillaries, estimating how large the diffusion capacities of the lungs and muscles must be to match the observed oxygen use at each virtual altitude step.
How lungs and muscles adapt as the air thins
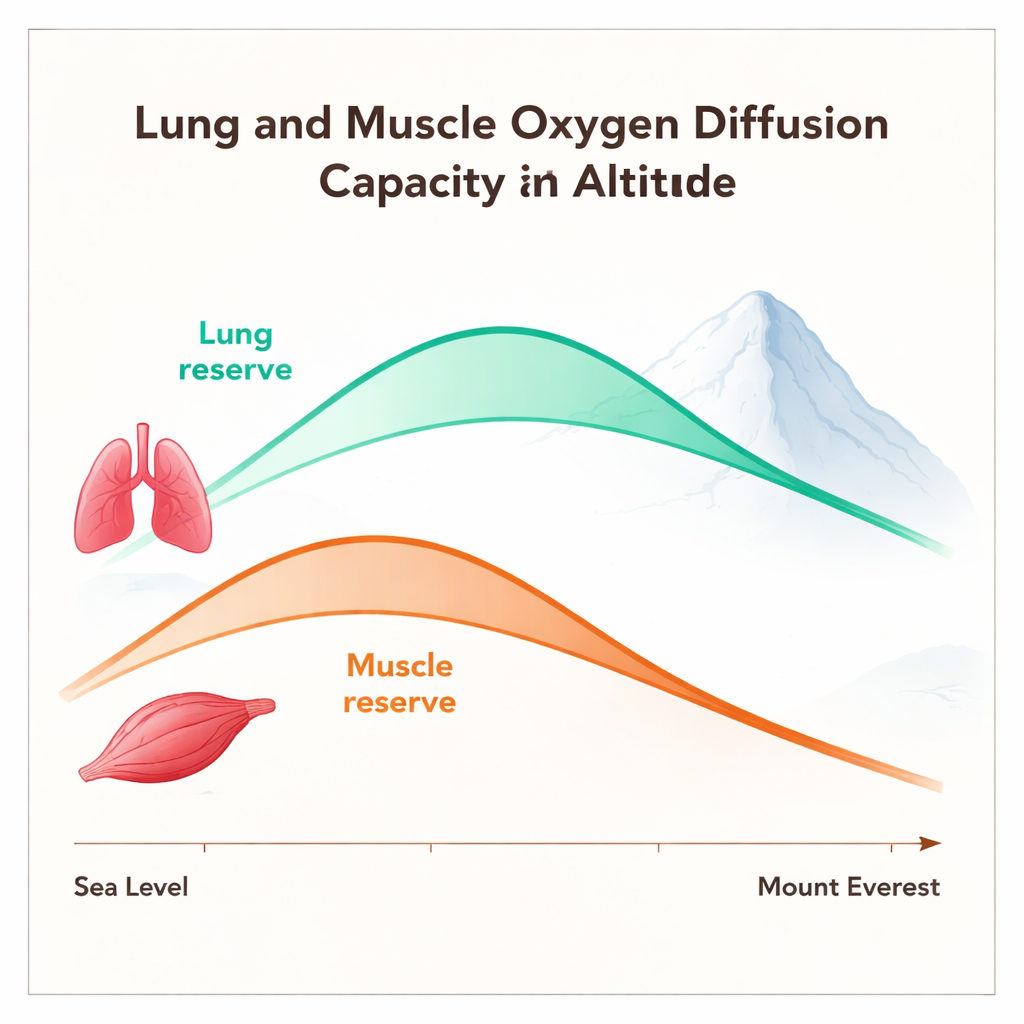
The model revealed a striking pattern. As altitude increases, the lung’s ability to diffuse oxygen does not simply decline. Instead, lung diffusion capacity rises from sea level to about 5,500 meters—roughly the highest altitude of permanent human settlements—before dropping again toward Everest’s summit. Even at the top, however, the lungs still appear to diffuse oxygen better than at sea level. In contrast, muscle diffusion capacity peaks earlier, around 3,500 meters, and then steadily falls. By the height of Everest, muscle diffusion capacity is predicted to be lower than at sea level. These “inverted U‑shaped” curves suggest that both lungs and muscles have a built‑in diffusion reserve, but the muscle reserve is exhausted at a lower altitude than the lung reserve.
What shapes these hidden reserves
To see which factors matter most, the team tested how sensitive the diffusion estimates were to small changes in key inputs such as blood flow, oxygen pressure in the lungs and arteries, venous oxygen levels, and hemoglobin. Lung diffusion capacity was strongly influenced by the oxygen pressure in the air sacs of the lungs and in arterial blood, especially at very high altitude, reinforcing the idea that gas exchange in the lungs becomes increasingly critical as the air thins. Muscle diffusion capacity was more affected by oxygen pressure in venous blood and by how much oxygen remained to drive movement into the mitochondria, the cell’s power plants. The model also showed that assumptions about the tiny oxygen pressure inside mitochondria and about hemoglobin’s affinity for oxygen can shift the absolute values and the altitude at which the peaks occur, but they do not change the overall pattern.
Limits, applications, and real‑world relevance
Because the study is a theoretical reconstruction based on many different expeditions and mostly male participants, its exact numbers should be viewed as estimates rather than precise measurements. The model also simplifies local details such as temperature, acidity, and uneven blood flow, all of which can affect oxygen transfer. Nonetheless, it offers a unified picture of how diffusion in lungs and muscles might change from sea level to extreme altitude. Clinically, similar approaches—using basic exercise tests, blood samples, and simple cardiac measurements—could help doctors estimate whether a patient’s exercise limitation stems more from pumping and delivering oxygen or from diffusing it into tissues.
What this means in everyday terms
For a layperson, the takeaway is that the body initially fights thin air by making the lungs and muscles better at drawing oxygen out of the blood, but this strategy has limits. Up to moderate and high altitudes, both lungs and muscles can ramp up their diffusion capacity, creating a helpful “reserve.” Beyond that, especially near the altitude of Everest, the muscles appear to hit a wall: even if the lungs are still doing relatively well, oxygen has trouble making the final jump into the working fibers. This imbalance helps explain why extreme altitude feels so exhausting and why performance drops so sharply, and it hints that protecting or boosting muscle oxygen diffusion could be key for climbers, athletes, and some patients facing low‑oxygen conditions.
Citation: Bourdillon, N., Manferdelli, G., Raberin, A. et al. Modelling lung and muscle oxygen diffusion capacities from sea-level to Mount Everest. Sci Rep 16, 7817 (2026). https://doi.org/10.1038/s41598-025-32441-9
Keywords: high altitude physiology, oxygen transport, lung diffusion, muscle oxygenation, Mount Everest