Clear Sky Science · en
Automated Global Positioning Layout (GPL) for accuracy assessment in CAD-CAM mandibular reconstruction – Method validation
Why this matters for jaw surgery
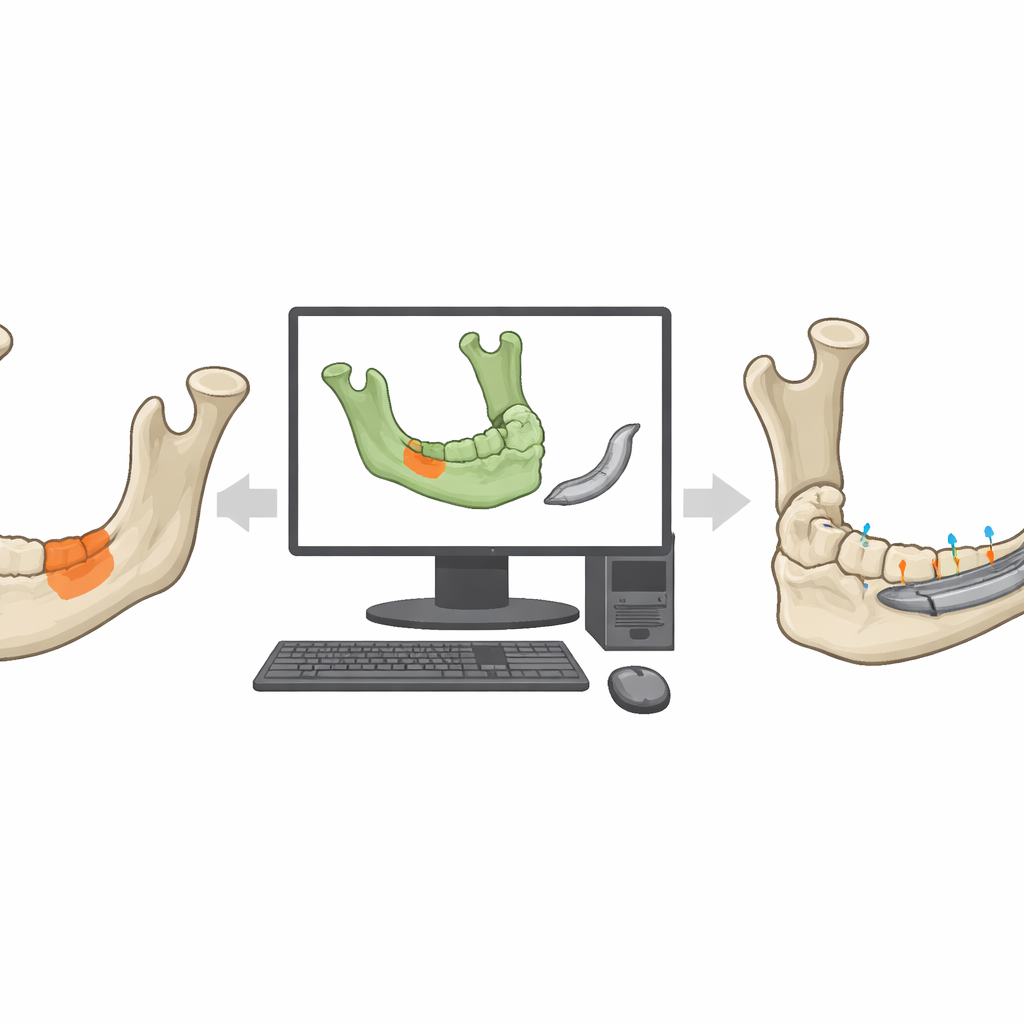
When part of a person’s lower jaw must be rebuilt, surgeons now rely on computer-guided planning and custom-made metal parts to restore appearance and chewing function. Yet doctors still lack a simple, consistent way to check how closely the final result matches the virtual plan. This study introduces and validates an automated method, called Global Positioning Layout (GPL), that measures how precisely a reconstructed jaw follows the 3D plan—offering a path toward safer, more predictable surgeries for patients.
Modern tools, missing yardstick
In head and neck surgery, computer-aided design and manufacturing let surgeons plan operations on detailed 3D models and create patient-specific titanium devices to rebuild the mandible. Virtual surgical planning helps decide exactly where to cut, how to shape the prosthesis, and how to position it. However, once surgery is done, there has been no widely accepted way to judge accuracy. Existing methods either depend heavily on the operator or hide important local errors. This lack of standardization makes it hard to compare results across hospitals, refine techniques, or link surgical precision to long-term outcomes such as biting, speaking, and appearance.
Three ways to measure a rebuilt jaw
The researchers focused on three approaches to compare the planned and postoperative jaws. The first, a traditional landmark-based method (Method A), asks an operator to pick specific points on the jaw—such as the tips of certain bony structures—and measure distances between them before and after surgery. Small changes in where those points are clicked can change the result, and some landmarks may be missing after large resections. The second, a surface-based method (Method B), digitally overlaps the two 3D jaw models and calculates how far apart the surfaces are on average and at their worst points. While more objective, it still needs manual alignment to get started and reports only non-directional distances, making it hard to know where and in which direction the jaw has shifted.
A new map for jaw position
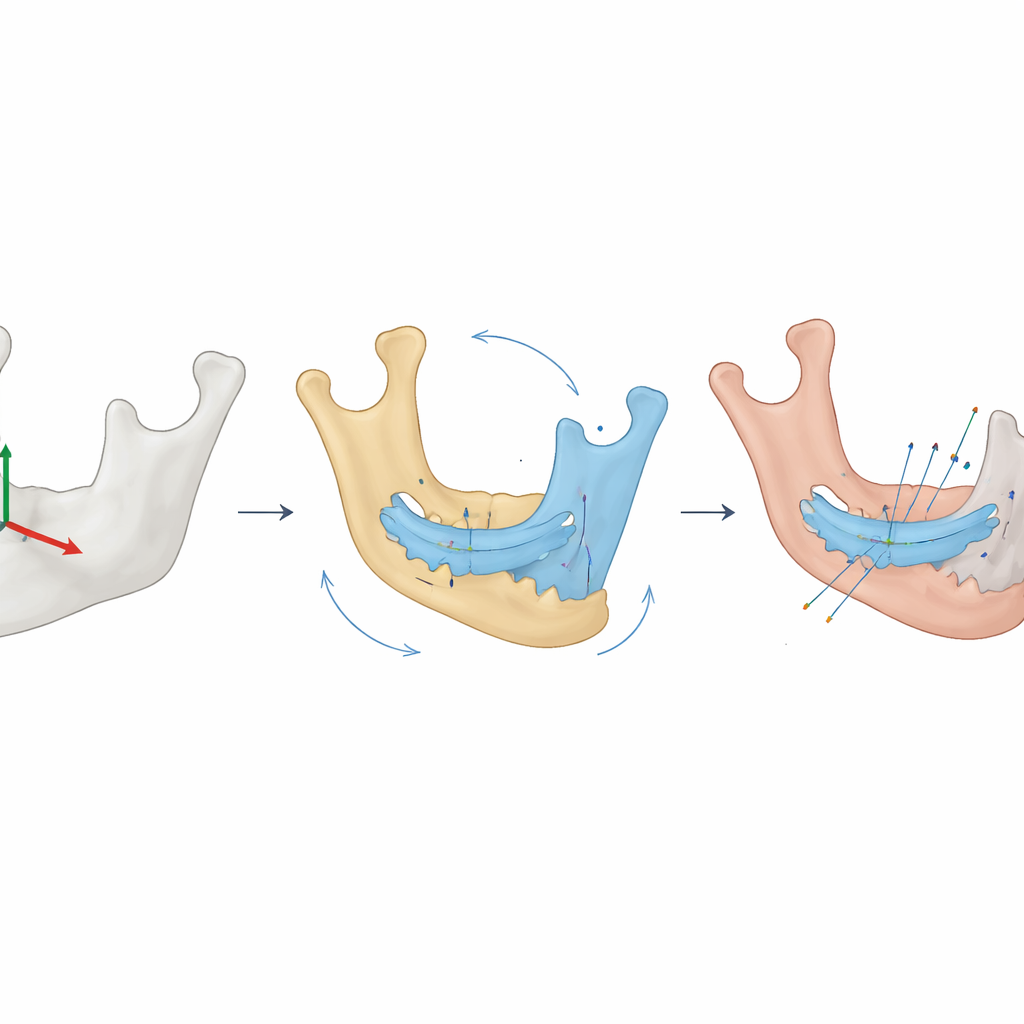
The new GPL method takes a different approach. It first creates a stable three-dimensional reference system based on a standard mandible shape, like fixing a map grid around the jaw. Both the planned reconstruction and the designed prosthesis are positioned within this common frame. Then the postoperative prosthesis is automatically aligned to the planned one, and this same movement is applied to the postoperative jaw. From these steps, the method calculates how much the reconstructed jaw has rotated and shifted along three axes. The entire workflow is automated, so once the models are loaded, the computer produces the measurements without operators choosing points or adjusting alignments by hand.
Testing reliability in real patients
To see how these methods perform in practice, the team analyzed 17 patients who received custom-made titanium devices to rebuild the mandible. Three different operators repeated all measurements on two separate occasions. GPL delivered identical numbers every time, regardless of who ran the analysis or when—showing complete reproducibility. The method revealed very small shifts: less than half a millimeter of translation on average and about one degree of rotation, well within ranges generally considered clinically negligible. In contrast, the landmark-based method showed wide variation within and between operators, and could not even be applied in some patients when key anatomical points were missing. The surface-based method produced stable mean distances, but still depended on manual initial alignment and could hide large local mismatches despite a reassuring overall average.
What this means for patients
The authors conclude that GPL is a robust, fully reproducible way to measure how closely a reconstructed jaw matches its computer plan, capturing both shifts and tilts in three dimensions. By removing operator subjectivity and working even when landmarks are missing, it offers a stronger foundation for comparing surgical techniques, improving device designs, and, ultimately, defining how much error is acceptable without harming function or appearance. As larger, multi-center studies adopt GPL and link its metrics to long-term patient outcomes, surgeons may gain clear, evidence-based targets for precision in computer-assisted mandibular reconstruction.
Citation: Vargiu, E., Tognin, L., Bettini, G. et al. Automated Global Positioning Layout (GPL) for accuracy assessment in CAD-CAM mandibular reconstruction – Method validation. Sci Rep 16, 9590 (2026). https://doi.org/10.1038/s41598-025-30516-1
Keywords: mandibular reconstruction, computer-assisted surgery, virtual surgical planning, 3D accuracy assessment, patient-specific implants