Clear Sky Science · en
Axillary surgery in patients with sentinel node macrometastases: secondary results of the randomized INSEMA trial
Why this matters for people with breast cancer
For many people diagnosed with early breast cancer, one of the biggest worries is how treatment will affect long‑term health and quality of life. Surgery to remove lymph nodes from the armpit can help doctors understand if cancer has spread, but it can also lead to arm swelling, stiffness, and pain that may last for years. This study from the large INSEMA trial asks a key question: can some women safely avoid more extensive underarm surgery—and its side effects—without sacrificing their chances of staying cancer‑free?
Two different ways to check the underarm
When cancer first appears in the breast, it often spreads—if at all—to a small number of “sentinel” lymph nodes in the armpit. Surgeons can remove just these few nodes in a procedure called sentinel lymph node biopsy. If cancer cells are found there, the traditional next step has been a bigger operation called completion axillary lymph node dissection, which removes many more nodes. The INSEMA study focused on women with small to medium‑sized breast tumors who had one to three sentinel nodes containing sizeable cancer deposits (macrometastases) and were treated with breast‑conserving surgery and whole‑breast radiation. It asked whether skipping the larger node removal was just as safe as doing it.
What the researchers did
Nearly 500 women from more than 100 hospitals in Germany and Austria agreed to be randomly assigned to one of two groups: one had only the sentinel node biopsy, and the other had the biopsy plus full removal of additional underarm nodes. After carefully excluding women whose treatment did not match the assigned plan or who did not receive radiation, 386 patients were analyzed in detail. All women had standard follow‑up care, including modern breast radiation and, when needed, hormone therapy, chemotherapy, and targeted drugs. The researchers then tracked how long women lived without the cancer returning or a new serious cancer appearing, a combined measure known as invasive disease‑free survival.
What the study found about cancer control
After a median of just over six years of follow‑up, both groups did well. In the group that had only the sentinel nodes removed, about 87 out of 100 women were free of invasive cancer problems at five years, compared with about 94 out of 100 in the group with more extensive node removal. Statistically, this difference was just shy of the cutoff the researchers had set to call it clearly significant, in part because the study ended up much smaller than originally planned. Importantly, deaths and overall survival were very similar: roughly 95–96 out of 100 women in both groups were alive at five years. Local relapses in the breast or underarm were rare in both groups, and underarm recurrences were almost nonexistent, suggesting that modern radiation and drug treatments are doing much of the heavy lifting in controlling microscopic disease.
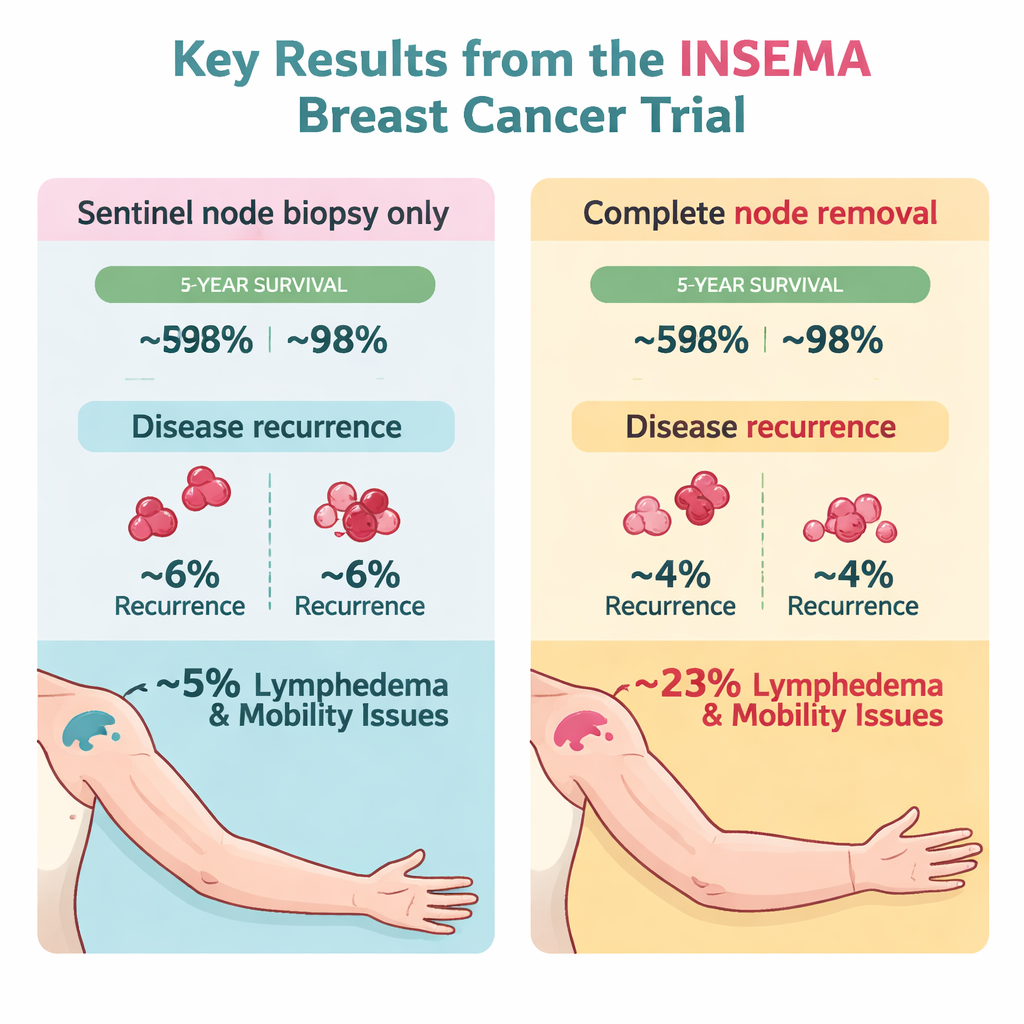
Balancing side effects and benefits
Where the two approaches clearly differed was in long‑term side effects. Women who avoided the larger underarm operation had lower rates of lasting arm swelling (lymphedema), less restriction in shoulder movement, and less arm and shoulder pain at their latest follow‑up visit. The authors also note that more women and doctors declined to proceed with full node removal when randomization assigned it, reflecting a growing reluctance to accept the added risks of this surgery. At the same time, there were hints that women whose tumors grew more quickly (high Ki‑67, a measure of cell division) might gain more protection from the bigger operation, though these findings come from small subgroups.
What this means going forward
Overall, this secondary analysis of the INSEMA trial did not show a clear survival advantage for routinely removing many additional underarm lymph nodes in women with one to three involved sentinel nodes who receive breast‑conserving surgery, whole‑breast radiation, and modern systemic therapy. Because the study was underpowered—far fewer women were enrolled than planned—the researchers caution that they cannot definitively prove that skipping the larger operation is just as good in every respect. Still, taken together with other recent trials, their results support a continued move toward less aggressive underarm surgery for many patients, reserving more extensive node removal for selected higher‑risk cases where the potential benefit may justify the added long‑term burden.
Citation: Reimer, T., Stachs, A., Veselinovic, K. et al. Axillary surgery in patients with sentinel node macrometastases: secondary results of the randomized INSEMA trial. npj Breast Cancer 12, 19 (2026). https://doi.org/10.1038/s41523-026-00902-7
Keywords: breast cancer surgery, sentinel lymph node, axillary lymph node dissection, lymphedema, radiation therapy