Clear Sky Science · en
The association between local therapies and survival among patients with metastatic inflammatory breast cancer
Why this matters to patients and families
When breast cancer has already spread throughout the body, doctors often focus on medicines that circulate in the bloodstream, such as chemotherapy. But for a rare, aggressive form called inflammatory breast cancer, the tumor in the breast and nearby tissues can still cause major problems. This study asks a practical question that many patients and families face: if the cancer is already metastatic, is it still worthwhile to go through surgery and radiation on the breast itself, or is chemotherapy alone enough?
Understanding this aggressive breast cancer
Inflammatory breast cancer is one of the most fast-moving types of breast cancer. It often does not form a typical lump; instead, the breast can look swollen, red, and warm, as if it is infected. Because it spreads early, about one in three patients are first diagnosed only after the cancer has already reached distant organs. Historically, doctors sometimes skipped local treatments like surgery or radiation for these patients, assuming that treating just the breast would not help someone whose cancer was already widespread. At the same time, newer cancer treatments have improved survival for many patients with metastatic disease, raising fresh interest in whether carefully chosen local treatments might add further benefit.
How the researchers studied treatment choices
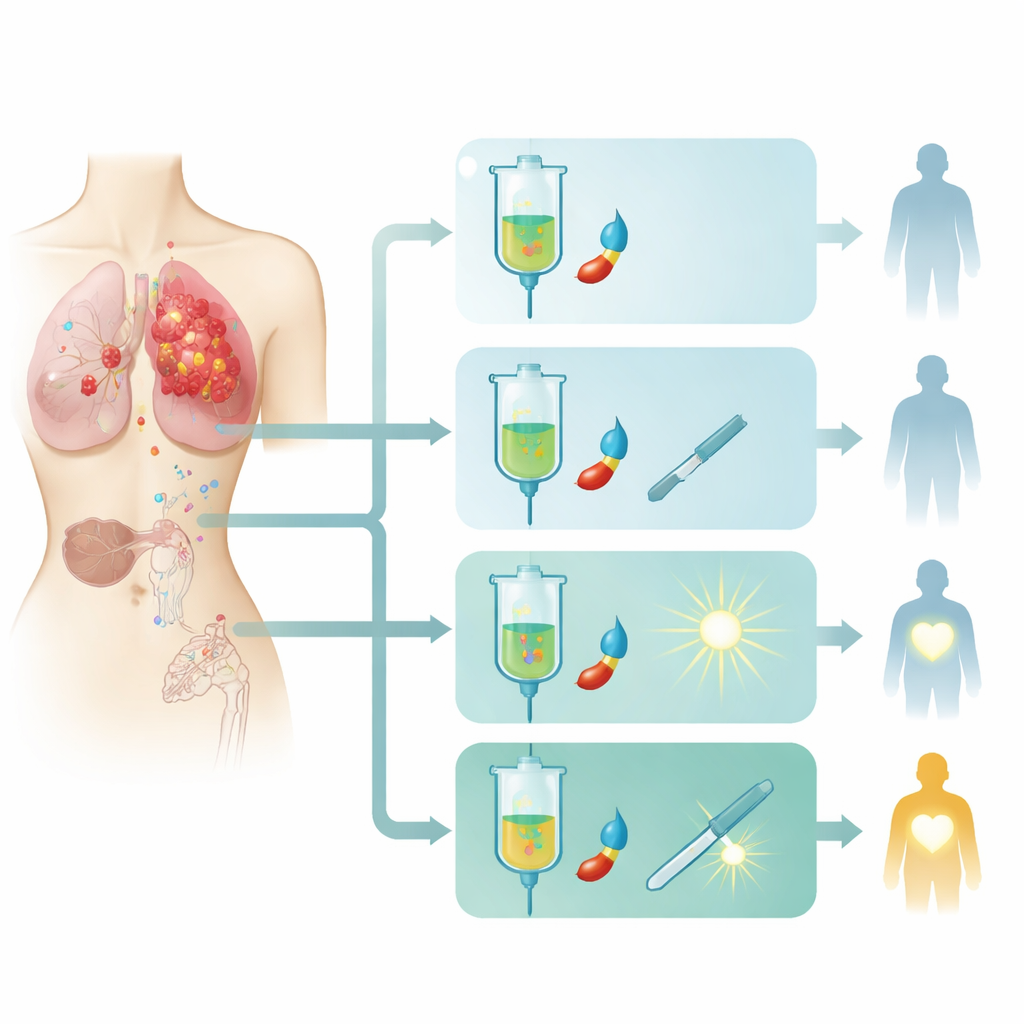
The researchers used a large national hospital database covering about 70% of new cancers in the United States. They identified 3219 women diagnosed between 2010 and 2021 with metastatic inflammatory breast cancer who received chemotherapy. Patients fell into four groups based on additional treatment: chemotherapy alone; chemotherapy plus breast surgery; chemotherapy plus radiation to the breast area; or "trimodality" care, meaning chemotherapy followed by surgery and then radiation. The team tracked how long patients lived after starting chemotherapy and used statistical methods to account for differences such as age, other illnesses, tumor biology, and how many organs the cancer had reached.
What the survival patterns showed
At first glance, survival seemed best for patients who received all three treatments, with about two-thirds alive at two years, compared with about half of those who had chemotherapy alone. However, once the researchers adjusted for the fact that doctors tend to offer more aggressive therapies to younger and healthier patients with less widespread disease, the picture changed. Surgery plus chemotherapy remained linked to better survival than chemotherapy alone, but adding radiation on top of surgery did not clearly extend life. Likewise, giving chemotherapy plus radiation without surgery did not improve survival compared with chemotherapy alone.
Clues about who might benefit from radiation
The team looked more closely at subgroups to see whether radiation might still help certain patients. One important signal came from women whose breast surgery did not fully remove all cancer, leaving positive margins at the edge of the removed tissue. In this smaller group, adding radiation after surgery and chemotherapy was associated with better survival, suggesting that radiation might help control remaining cancer in the breast area when surgery cannot achieve a clean removal. On the other hand, when patients were grouped by tumor type, lymph node involvement, age, or how well they responded to chemotherapy before surgery, radiation generally did not show a clear survival advantage.
What this means for treatment decisions
For people facing metastatic inflammatory breast cancer, these findings suggest that surgery to remove the breast tumor, when added to chemotherapy, may be linked to longer life, while routine radiation after surgery does not appear to boost survival for most patients. Radiation may still be important for a select group, especially when surgeons cannot fully clear the tumor. The study cannot prove cause and effect, and it does not capture other reasons to consider local treatment, such as preventing painful or hard-to-control tumors in the breast. Still, it provides large-scale evidence to help patients and doctors weigh the extra burden of surgery and radiation against the potential benefits, and it highlights the need for more focused trials to clarify when added radiation truly makes a difference.
Citation: Jitwatcharakomol, T., Gokun, Y., Walston, S.A. et al. The association between local therapies and survival among patients with metastatic inflammatory breast cancer. npj Breast Cancer 12, 35 (2026). https://doi.org/10.1038/s41523-026-00899-z
Keywords: inflammatory breast cancer, metastatic breast cancer, breast surgery, radiation therapy, cancer survival