Most people infected with the tuberculosis (TB) bacterium never fall ill, yet TB remains a leading infectious killer. Doctors know that certain immune cells, called T cells, help control the germ Mycobacterium tuberculosis (Mtb), but they have struggled to pin down exactly which T cells matter most. This study uses the familiar tuberculin skin test—the small bump raised on the forearm after a TB test—as a window into how human T cells respond to Mtb in real time, and introduces a new way to find shared, Mtb‑targeting T cell patterns across different people.
From simple skin test to powerful immune model
The tuberculin skin test (TST) has long been used in clinics as a yes‑or‑no readout of prior TB exposure: a small shot of purified TB proteins under the skin, then measuring the bump two to three days later. The authors turned this routine test into a research tool by taking tiny biopsies from the injection site at day 2 and day 7, and comparing them to saline control injections. They measured which genes were turned on and, crucially, sequenced the T cell receptors (TCRs)—the molecular “ID cards” that let each T cell recognize a specific target. This allowed them to follow how the local immune response matured over time, rather than just recording the size of the bump.
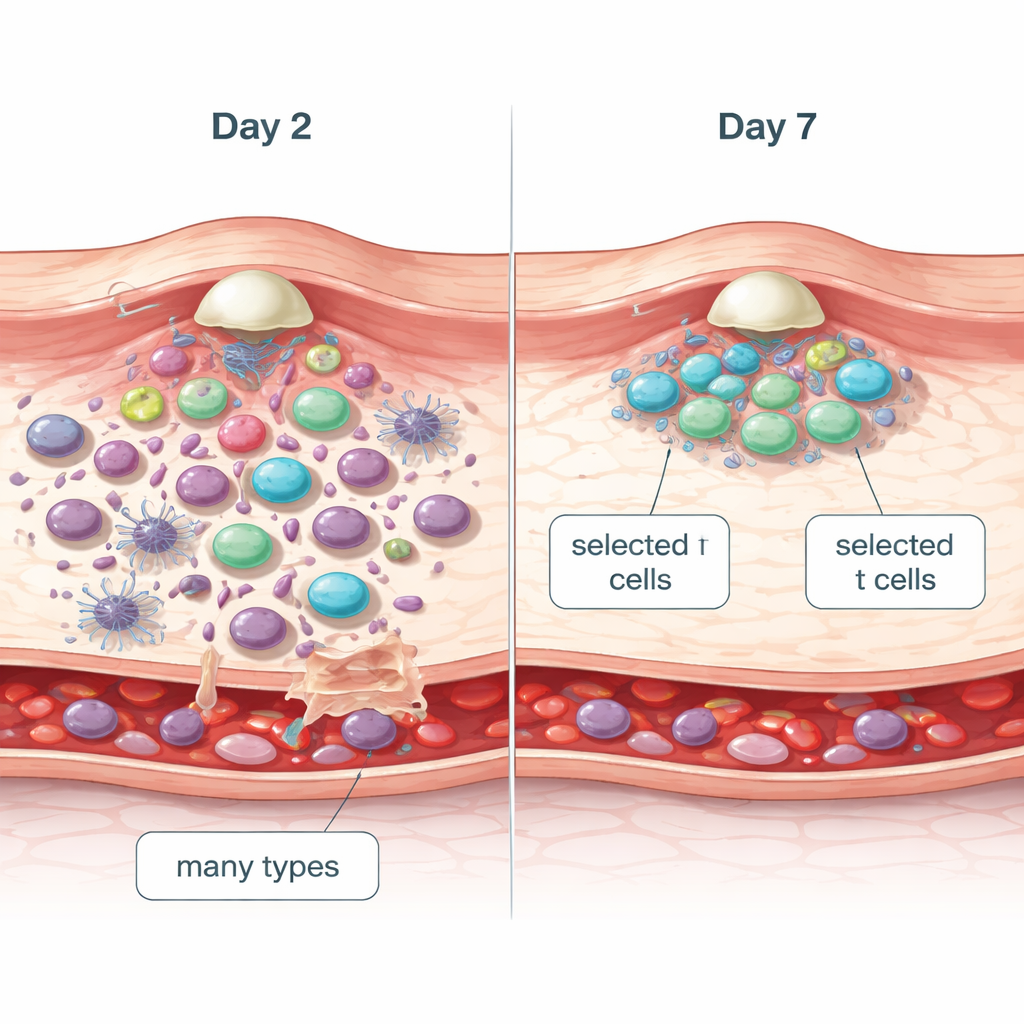
Early crowd, later specialists Figure 1.
Gene‑expression data showed that by day 2 the skin was already inflamed and packed with many types of immune cells, but there was little sign of cell division. By day 7, the overall inflammatory signals had started to quiet down, while genes linked to the cell cycle and proliferation were strongly increased, especially in CD4 T cells. TCR sequencing confirmed this shift: at day 2, the T cell population at the test site was diverse and only mildly skewed toward any particular clones, suggesting fairly non‑selective recruitment from the blood. By day 7, a smaller set of T cell clones had expanded dramatically—an “oligoclonal” pattern—indicating that T cells recognizing TB antigens were selectively proliferating at the site.
Proving the T cells really recognize TB
To verify that these expanding clones were truly responding to TB, the team compared skin TCR sequences to large public databases of TCRs with known specificities, and to T cells grown in the lab by stimulating volunteers’ blood cells with TB proteins. Day‑7 skin samples were highly enriched for TCRs that reacted to TB, and depleted for TCRs known to target unrelated viruses such as CMV and EBV. Importantly, many of the TB‑reactive TCRs found in each person’s skin test were “private” sequences—unique to that individual and not shared with others—highlighting why simple counting of TB‑reactive T cells in blood has struggled to predict who is protected or at risk.
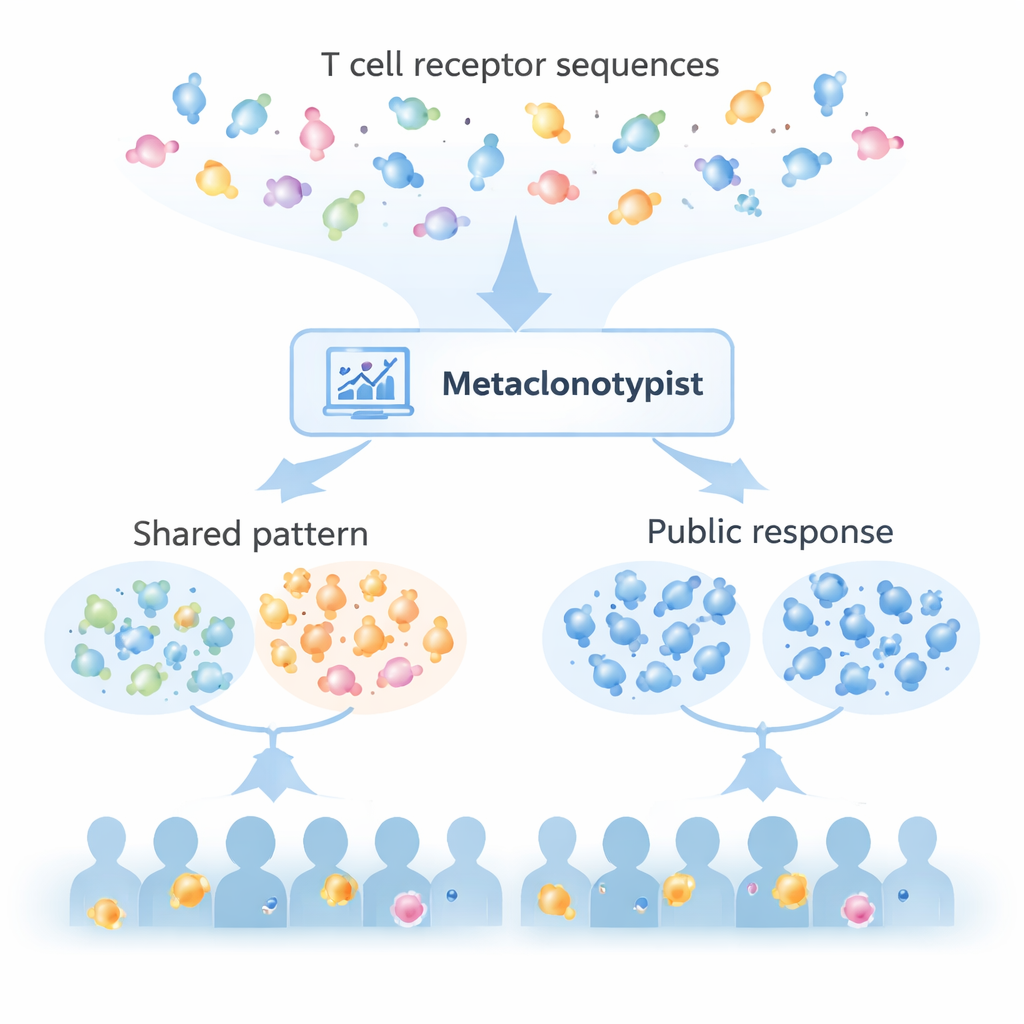
Finding shared immune patterns with Metaclonotypist Figure 2.
Despite this individuality, the researchers reasoned that different people’s TCRs might still converge on the same TB peptide targets, even if the exact receptor sequences differ slightly. They built a computational pipeline, Metaclonotypist, to group similar TCRs into “metaclones”—clusters predicted to recognize the same piece of TB protein presented by a particular HLA molecule (the immune system’s display frame). By analyzing day‑7 skin TCRs from over 150 participants, they discovered 180 such metaclones, the vast majority linked to class II HLA molecules that present antigens to CD4 T cells. Only about 3% of unique TCR sequences fell into these public metaclones, but more than 95% of participants contributed to at least one of them, and as few as 10 highly “public” metaclones were enough to detect TB‑reactive T cells across the whole cohort.
Shared signatures across tissues and diseases
To test whether these metaclones really marked TB responses rather than just any inflammation, the authors checked for them in independent datasets. The same metaclones were enriched in TB‑reactive T cells grown from blood, in blood and lung tissue from TB patients compared to people with cancer or COVID‑19, and at lung disease sites compared to the patients’ own blood. In contrast, the full set of expanded TCRs from the day‑7 skin tests showed weaker enrichment, underscoring that metaclones capture the most TB‑specific, widely shared part of the response. This suggests that the skin test can serve as a practical, standardized “challenge” model for studying clinically relevant TB immunity in humans.
What this means for patients and vaccines
For non‑specialists, the key message is that the familiar TB skin test hides a rich, evolving story under the skin. The early bump reflects a general influx of immune cells, but by day 7 the site is dominated by a focused set of CD4 T cells actively recognizing TB proteins. Most of these responding cells are unique to each person, yet the Metaclonotypist approach reveals a small number of shared T cell patterns—metaclones—that appear again and again across many people and in diseased lungs. These public signatures could form the basis of future blood tests to stratify TB risk, track treatment, or assess vaccines, and may point the way to specific TB peptides that elicit the most protective T cell responses.
Citation: Turner, C.T., Tiffeau-Mayer, A., Rosenheim, J. et al. Evolution of the tuberculin skin test reveals generalisable Mtb-reactive T cell metaclones.
Nat Commun17, 1900 (2026). https://doi.org/10.1038/s41467-026-68678-9
Keywords: tuberculosis, T cells, tuberculin skin test, T cell receptor sequencing, immune biomarkers