Clear Sky Science · en
Unbiased clustering of acute-on-chronic liver failure patients using machine learning in a real-world ICU cohort
Why this matters for people with liver disease
When people with long-standing liver disease suddenly become very sick, doctors must quickly judge who is at greatest risk of dying and who might recover. Today, those decisions rely on scoring systems built from expert opinion and small studies. This paper shows how a data-driven, machine learning approach can uncover hidden patterns in real-world intensive care unit (ICU) patients with acute-on-chronic liver failure, potentially pointing to simpler, more accurate ways to identify who needs the most aggressive care.
Sorting very sick patients without prior assumptions
The researchers studied 1,256 ICU patients with acute-on-chronic liver failure, defined by North American criteria that focus on failures of the brain, lungs, heart and circulation, and kidneys. Instead of starting from established liver scores, they fed 50 routinely measured clinical and laboratory values into an unsupervised machine learning method called nonnegative matrix factorization. This technique looks for natural groupings in the data without being told ahead of time which features are important or how many patient types to expect. A separate algorithm was used to test different solutions and decide how many clusters best fit the data.
Two clear groups with very different outcomes
Across multiple variants of the clustering method, the data consistently split best into just two patient groups. The winning model, known as the Lee algorithm, produced highly stable clusters: the same patients tended to be grouped together even when the model was re-run many times. When the authors compared survival, they found striking differences. One cluster had a 30-day death rate of about 70%, while the other had a rate of about 26%. This simple two-cluster scheme predicted mortality better than the traditional approach of counting how many organs had failed, even though both groups contained patients with a mix of organ failures.
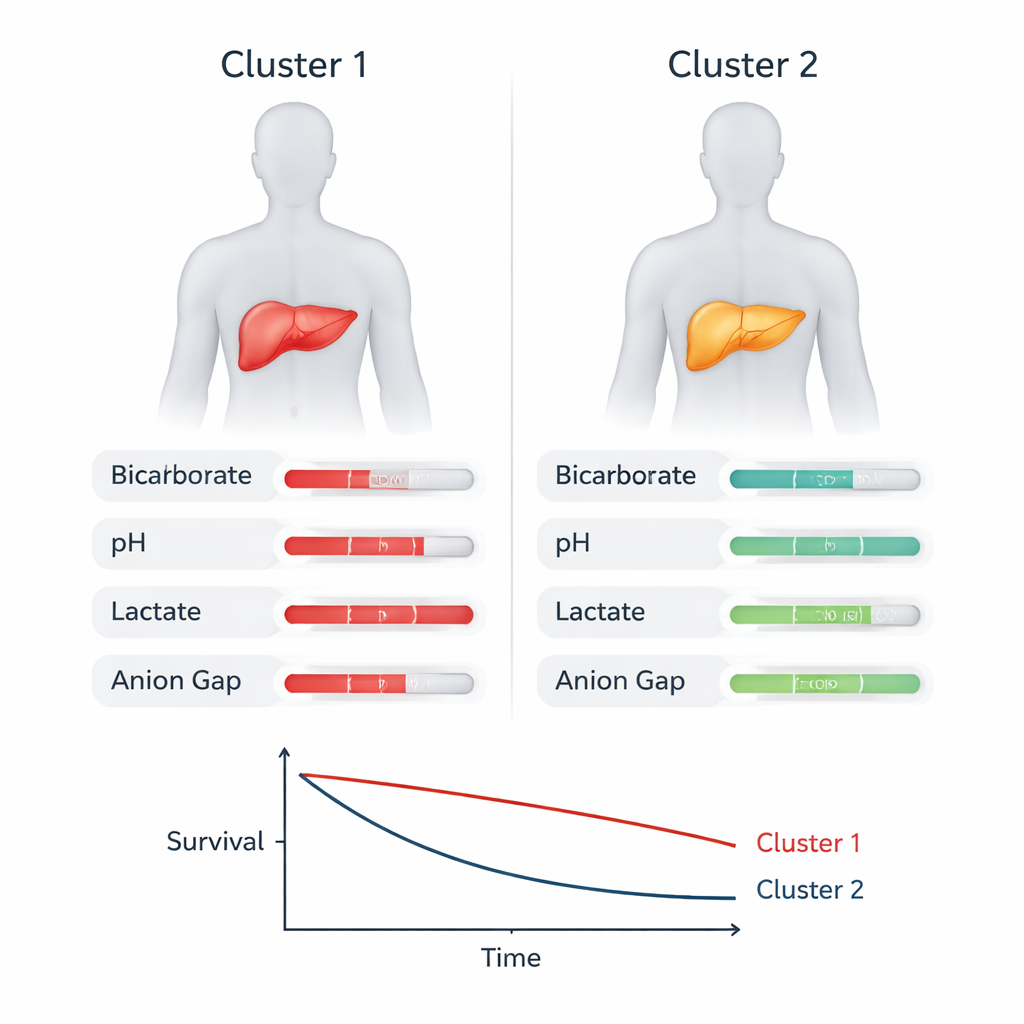
Blood chemistry and metabolism as key signals
To understand what separated the clusters, the team examined which measurements most strongly drove the grouping. Several familiar markers of critical illness, such as the need for blood pressure drugs, blood lactate levels, and creatinine (a kidney function marker), were important. But a particularly notable finding was that measures of acid–base balance in the blood—bicarbonate, pH, base excess, lactate, and the anion gap—were among the top contributors. The high-risk cluster tended to have more severe acid–base disturbances: lower pH and bicarbonate, larger base deficits, and higher anion gaps, consistent with widespread metabolic stress and poor tissue oxygenation. These patterns suggest that how well the body maintains its chemical balance may be just as important as which organs have failed.
Testing the pattern in other patient groups
Because ICU data come from a single health system and one definition of acute-on-chronic liver failure, the authors checked whether their findings held up elsewhere. They applied the same model to patients meeting a European definition of the syndrome and to a broader group of ICU patients with decompensated cirrhosis, many of whom did not formally qualify as having acute-on-chronic liver failure. In both settings, the clustering again split patients into two groups with similarly large gaps in 30-day mortality, and the same acid–base related variables remained central. An independent ICU database from many U.S. hospitals, though lacking long-term outcome data, showed the same two-cluster structure and overlapping key variables, supporting the robustness of the approach.
What this could mean for future care
The study does not yet deliver a bedside tool that directly improves survival, and it has limitations, including its focus on very sick ICU patients and reliance on retrospective data. Still, it offers a proof of concept that an unbiased, data-driven method can reveal clinically meaningful subtypes within a complex condition that has long resisted simple classification. For patients and families, the main message is that the balance of acids and bases in the blood—something doctors already measure routinely—may provide powerful clues about risk and recovery in severe liver crises. With further research and prospective testing, such clustering models could help clinicians identify the most fragile patients earlier and design treatments that target the metabolic disturbances driving their poor outcomes.
Citation: Zhang, M., Ji, F., Zu, J. et al. Unbiased clustering of acute-on-chronic liver failure patients using machine learning in a real-world ICU cohort. Nat Commun 17, 1670 (2026). https://doi.org/10.1038/s41467-026-68368-6
Keywords: acute-on-chronic liver failure, machine learning, ICU outcomes, acid-base balance, cirrhosis