Clear Sky Science · en
Mapping the barriers and facilitators of oral healthcare access for vulnerable migrants across high-income countries: a scoping review
Why healthy teeth matter for people on the move
For many people forced to move across borders—such as refugees, asylum seekers, and low‑paid migrant workers—bad toothache or bleeding gums often sit low on a long list of worries. Yet poor oral health can make it hard to eat, sleep, work, and even talk with confidence, and it is tied to serious diseases like heart problems and diabetes. This review looks at what helps and what blocks vulnerable migrants in wealthy countries from getting basic dental care, and why fixing these gaps is about fairness, not just fillings.

The hidden burden behind a simple toothache
Across high‑income countries, migrants facing hardship—people seeking asylum, undocumented workers, unaccompanied minors and those who have been trafficked—consistently have worse teeth and gums than the general population. Studies from Germany, for example, show far higher levels of untreated tooth decay among refugees than among local residents. Tooth problems are not just about pain: they affect speaking, eating, appearance, and self‑esteem, and are linked with long‑term conditions such as heart disease and diabetes. For those already dealing with trauma, low income, and unstable housing, the added weight of poor oral health deepens disadvantage.
How money, rules, and culture shape the dental journey
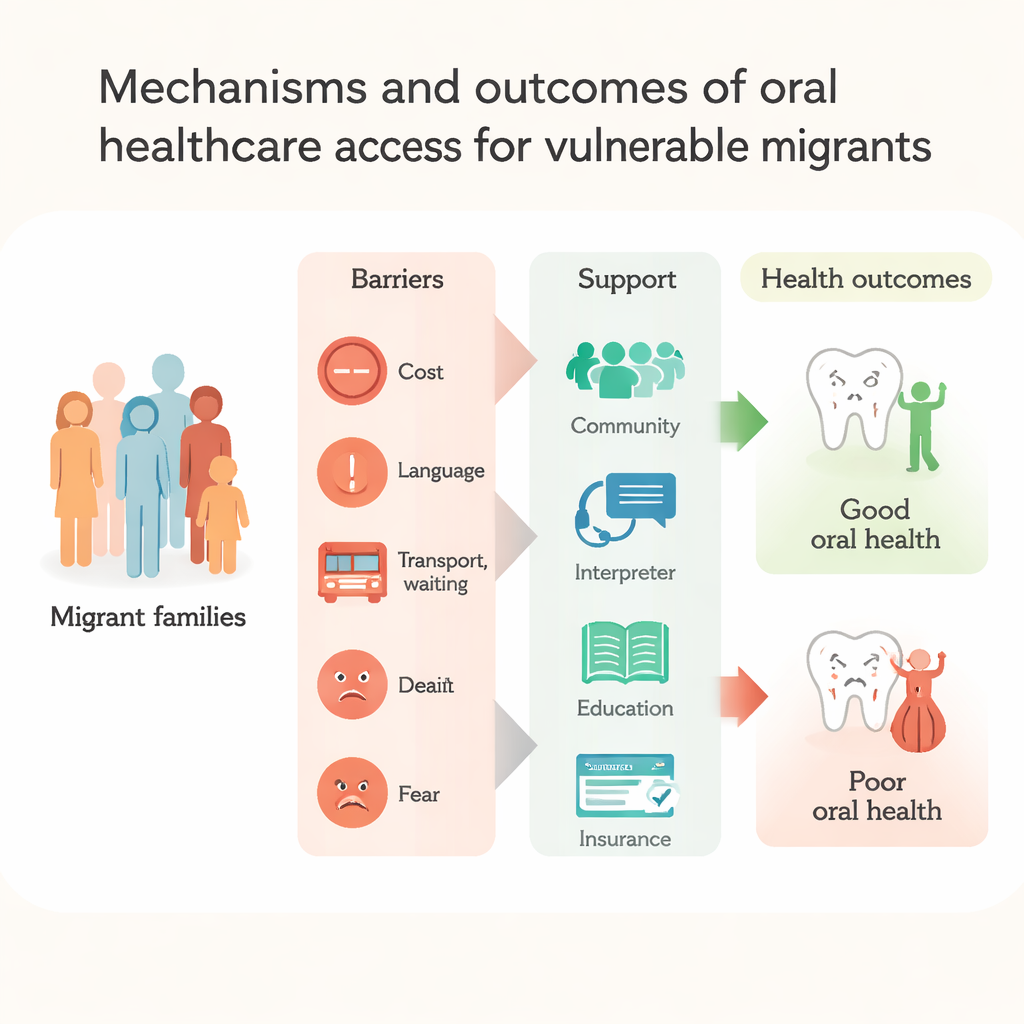
The authors examined 17 studies from eight rich countries and organised their findings using a well‑known public health model that looks at layers of influence around a person. At the broadest layer—money, policies, and social conditions—cost was the single most common barrier. Migrants often described dental care in host countries as unaffordable, even when they understood its importance. Confusing or limited insurance schemes meant people did not know what was covered, or could only get extractions instead of tooth‑saving treatments. Financial strain also pushed families toward cheaper, sugary foods and made it hard to pay for toothpaste, brushes, or travel to the clinic.
Everyday obstacles: language, transport, and trust
Closer to daily life, language difficulties loomed large. Many migrants struggled to book appointments, understand treatment plans, or explain symptoms. Interpreters, when available, could help, but some patients worried that key details were lost or that interpreters spoke on their behalf. Practical issues such as long journeys, confusing transport systems, unsafe clinic locations, and juggling work and childcare led to missed or delayed visits. Experiences of war, flight, and ongoing legal uncertainty pushed dental problems far down the priority list. On top of this, many reported feeling disrespected, judged, or discriminated against by dental staff, or described past mistakes such as the wrong tooth being removed. These encounters bred mistrust and fear, so people waited until pain became unbearable before seeking help.
Family roles, beliefs, and the power of community
Personal and social factors also played a strong part. Women, especially pregnant women and mothers, often put their children’s needs first and postponed their own treatment, even when they knew it mattered. In some cultures, men were expected to hide pain and avoid seeking care. Limited knowledge about prevention—such as the value of regular check‑ups or fluoride—meant people relied on home remedies or emergency visits rather than routine care. Yet the review also found hopeful signs: cultural and religious practices like using miswak sticks supported daily mouth cleaning for some groups, and spirituality gave people emotional strength to face health problems. Community networks, schools, migrant centres, and supportive dental clinics helped by providing interpreters, transport guidance, free or low‑cost check‑ups, and tailored health education that made local systems easier to navigate.
From blaming individuals to fixing the system
Overall, the review makes clear that poor dental health among vulnerable migrants is not the result of personal neglect alone. It arises from a web of structural barriers—high costs, patchy insurance, complex rules, language gaps, discrimination, and the strain of starting over in a new country. The authors argue that solutions must go beyond telling people to brush and floss. Instead, governments and health services should treat oral health as a public health priority, extend fair coverage for dental care, simplify access rules, and train providers in culturally sensitive, respectful care. When clinics, communities, and policies work together to remove these obstacles, migrants are far more likely to receive timely, preventive dental care—and a healthy mouth becomes a realistic part of building a new life.
Citation: Lal, Z., Silva, L., Alam, N. et al. Mapping the barriers and facilitators of oral healthcare access for vulnerable migrants across high-income countries: a scoping review. BDJ Open 12, 17 (2026). https://doi.org/10.1038/s41405-026-00398-0
Keywords: oral health, migrants, healthcare access, dental care, health inequalities