Most people think of scars as marks on the skin, but a similar scarring process can silently reshape our organs from the inside. This review explains how fibrosis—excessive internal scarring—develops in the lungs, heart, liver and kidneys, why it is now a major global health threat, and how new technologies and treatments might finally let doctors slow or even reverse it.
Scars That Threaten Organ Function
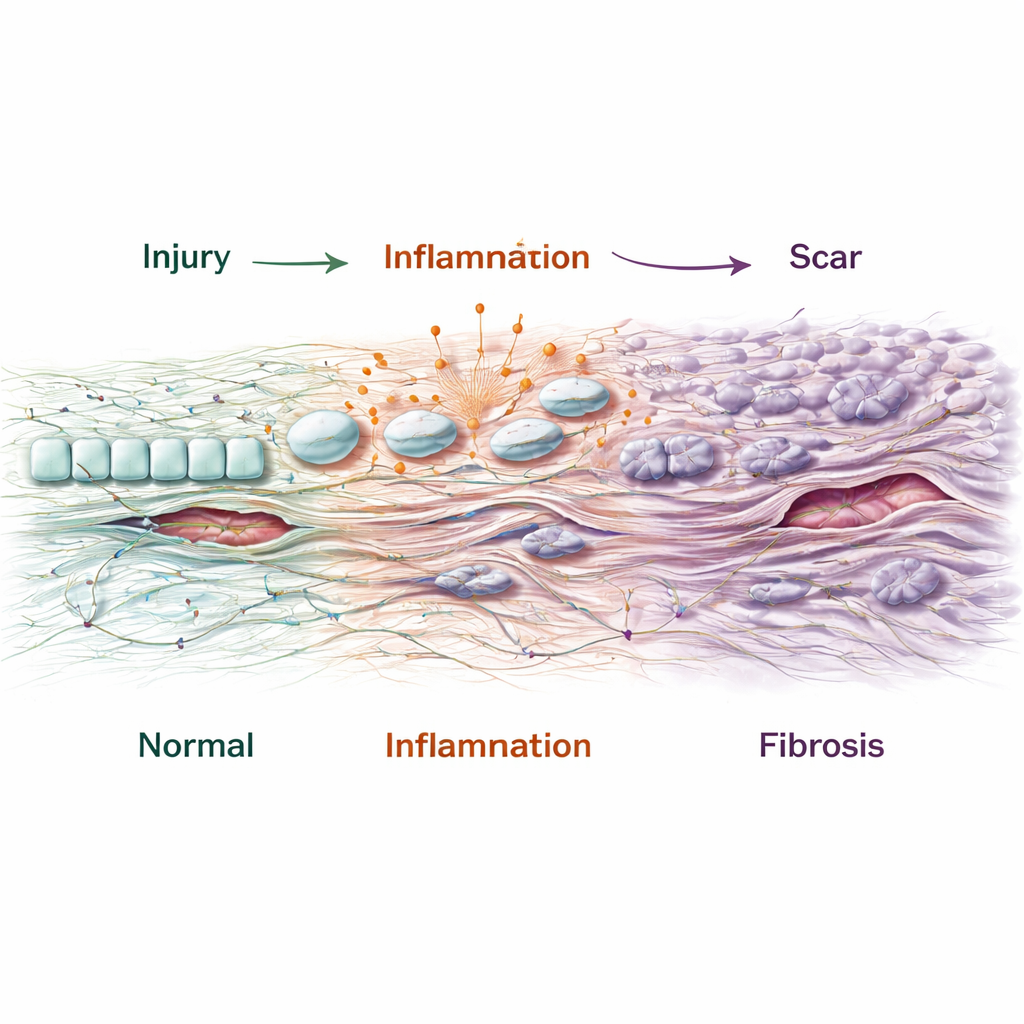
Fibrosis starts as the body’s attempt to repair damage. After an injury, cells lay down a mesh of proteins, such as collagen, to shore up weakened tissue. When damage is mild or short-lived, this process winds down and normal structure returns. But when injury is severe or repeated—because of infections, toxins, high blood pressure, excess fat, or immune attacks—the repair system becomes stuck in “on” mode. Layers of dense scar tissue accumulate, distort the organ’s architecture, and gradually choke off its function. The review notes that about a quarter of the world’s population is affected by fibrotic conditions, from idiopathic pulmonary fibrosis in the lungs to heart failure, cirrhosis of the liver, and chronic kidney disease. Yet only a handful of drugs, such as pirfenidone, nintedanib, resmetirom and semaglutide, are currently approved, and they mostly slow decline rather than undo existing scars.
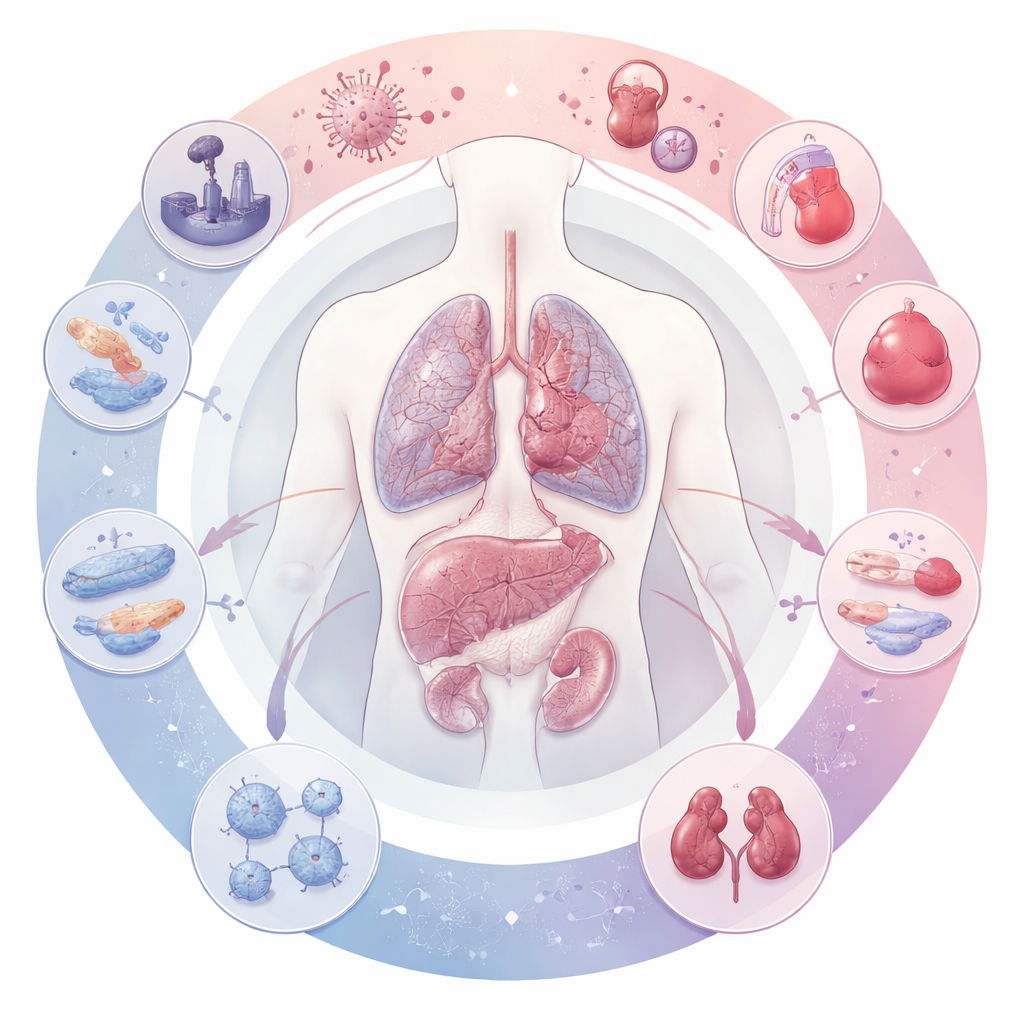
Many Cell Types, One Harmful Outcome Figure 1.
Scientists once blamed fibrosis mainly on fibroblasts, the cells that manufacture the extracellular “mesh” between cells. This article shows that the picture is far more complex. In each organ, several cell types can transform into aggressive scar-producing cells called myofibroblasts: surface-lining epithelial cells, blood-vessel endothelial cells and certain immune cells can all switch identity and start behaving like fibroblasts. At the same time, normal parenchymal cells (such as lung alveolar cells, heart muscle cells and hepatocytes in the liver) lose their specialized functions, become stressed or senescent, and release danger signals. Immune cells swarm in, pumping out inflammatory and growth factors. Over time, this tangled “fibrogenic niche”—a web of altered cells, signaling molecules and stiffened matrix—locks the organ into a cycle of chronic damage and scarring.
Different Organs, Shared Patterns
Although triggers vary by organ, the scarring story follows similar steps. In the lungs, inhaled particles, viral infections or radiation injure the delicate air sacs; the cells that normally regenerate the gas-exchange surface stall in a half-healed state and send out strong fibrotic signals. In the heart, heart attacks or long-standing pressure overload kill or stress heart muscle cells, and fibroblasts fill the gaps with stiff collagen that impairs pumping and disrupts electrical conduction. In the liver, chronic viral hepatitis, alcohol, or fat overload injure hepatocytes and activate stellate cells that sit between liver plates, turning them into collagen factories and reshaping blood flow through the organ. In the kidney, highly energy-dependent tubule cells respond to toxins or lack of oxygen by dying, becoming senescent, or reprogramming their metabolism, which in turn recruits immune cells and activates perivascular fibroblasts. Despite these differences, the end result is remarkably similar: narrowed vessels, distorted architecture and progressive loss of function.
Signaling Circuits and Emerging Therapies Figure 2.
Beneath these cellular dramas lie common signaling circuits—biochemical “wiring diagrams” that keep fibrosis going. The review highlights central pathways such as TGF-β, Wnt/β-catenin, MAP kinase, JAK–STAT, PI3K–AKT, integrins, and stress responses in the endoplasmic reticulum. These pathways govern whether cells proliferate, change identity, or secrete matrix. Because they are reused in many organs, drugs that modulate them could, in principle, treat fibrosis in multiple tissues. The authors catalogue dozens of experimental medicines in clinical trials: small molecules, antibodies and receptor blockers aimed at these core routes, alongside biologic therapies that mimic protective hormones such as FGF19 and FGF21. They also discuss more radical approaches, including chimeric antigen receptor (CAR) T cells and engineered macrophages designed to selectively eliminate overactive fibroblasts or stellate cells, and gene- or RNA-based strategies delivered by nanoparticles.
From Big Data to Personalized Anti-Scarring Drugs
A major theme of the article is the power of new research tools. Single-cell sequencing and spatial mapping now let scientists watch individual cells in diseased organs and see how they change over time and location. Multiomics approaches combine DNA, RNA, protein and metabolic data to define harmful and protective cell subtypes, such as particular fibroblast, endothelial or macrophage populations that appear again and again in different fibrotic diseases. At the same time, advanced organ models—3D organoids, organ-on-a-chip systems and living tissue slices—reproduce human-like scarring in the lab, allowing faster and more realistic drug testing. Artificial intelligence is being trained on these complex datasets to spot new drug targets, design molecules and even read biopsy slides more consistently than humans, offering more objective ways to diagnose and monitor fibrosis.
Why This Matters for Patients
To a lay reader, the central message is that fibrosis is not a vague, irreversible “wear and tear” phenomenon but a specific, multi-step process that can be measured and, increasingly, manipulated. By uncovering the shared rules by which normal repair turns into runaway scarring, and by mapping the key cell types and pathways involved, researchers are building the foundation for treatments that go beyond symptom relief. The authors envision a future in which combinations of targeted drugs, cell therapies and AI-guided diagnostics are tailored to each patient’s pattern of injury and scar formation, with the long-term goal of not just slowing fibrosis, but helping damaged organs truly heal.
Citation: Chen, X., Zhang, J., Guo, L. et al. Decoding organ fibrosis: mechanistic insights and emerging therapeutic strategies.
Sig Transduct Target Ther11, 82 (2026). https://doi.org/10.1038/s41392-025-02532-0