Clear Sky Science · en
Hypertension pharmacogenetics and limitations in Africa – a focus on the ACE, AGTR1 and CYP2C9 genes
Why Blood Pressure Medicines Do Not Work the Same for Everyone
High blood pressure is often called a “silent killer,” and this is especially true in many African countries, where rates of hypertension and kidney disease are among the highest in the world. Yet even when people take their prescribed pills, many still do not reach healthy blood pressure levels. This article explains how inherited differences in our genes can change the way common blood pressure medicines work, why these effects may be especially important in Africans, and what needs to change so that treatment can be better tailored to each person.
High Blood Pressure, Kidneys, and Everyday Risk
Hypertension affects more than a billion adults worldwide and is particularly common in sub-Saharan Africa, where it often goes undiagnosed and undertreated. Over time, raised blood pressure damages the delicate lining of blood vessels, increasing the risk of heart attacks, strokes, and kidney failure. Kidney disease and hypertension feed into one another: as kidney function drops, blood pressure tends to rise, and as blood pressure rises, the kidneys are injured further. Other common conditions in Africa—including obesity, diabetes, tobacco use, and HIV infection—add to this load. Many people living with HIV also have high blood pressure, sometimes without knowing it, and certain genetic variants found almost only in people of African ancestry further raise the risk of kidney damage.
How Common Medicines Control Blood Pressure
Doctors often treat hypertension and kidney disease by blocking a hormone system that narrows blood vessels and makes the body retain salt and water. Two major types of drugs are used: ACE inhibitors, which prevent the formation of a strong vessel-tightening hormone, and ARBs, which stop this hormone from locking onto its main receptor on blood vessel walls. These drugs not only lower blood pressure but also protect the kidneys and heart. However, they must first be processed by the body. Some are converted in the liver into a more active form before they can work properly, and all of them rely on proteins in our bodies that either build or receive hormone signals. Differences in the genes that encode these proteins can therefore change both how well a medicine works and whether it causes side effects.
Key Genes That Shape Drug Response
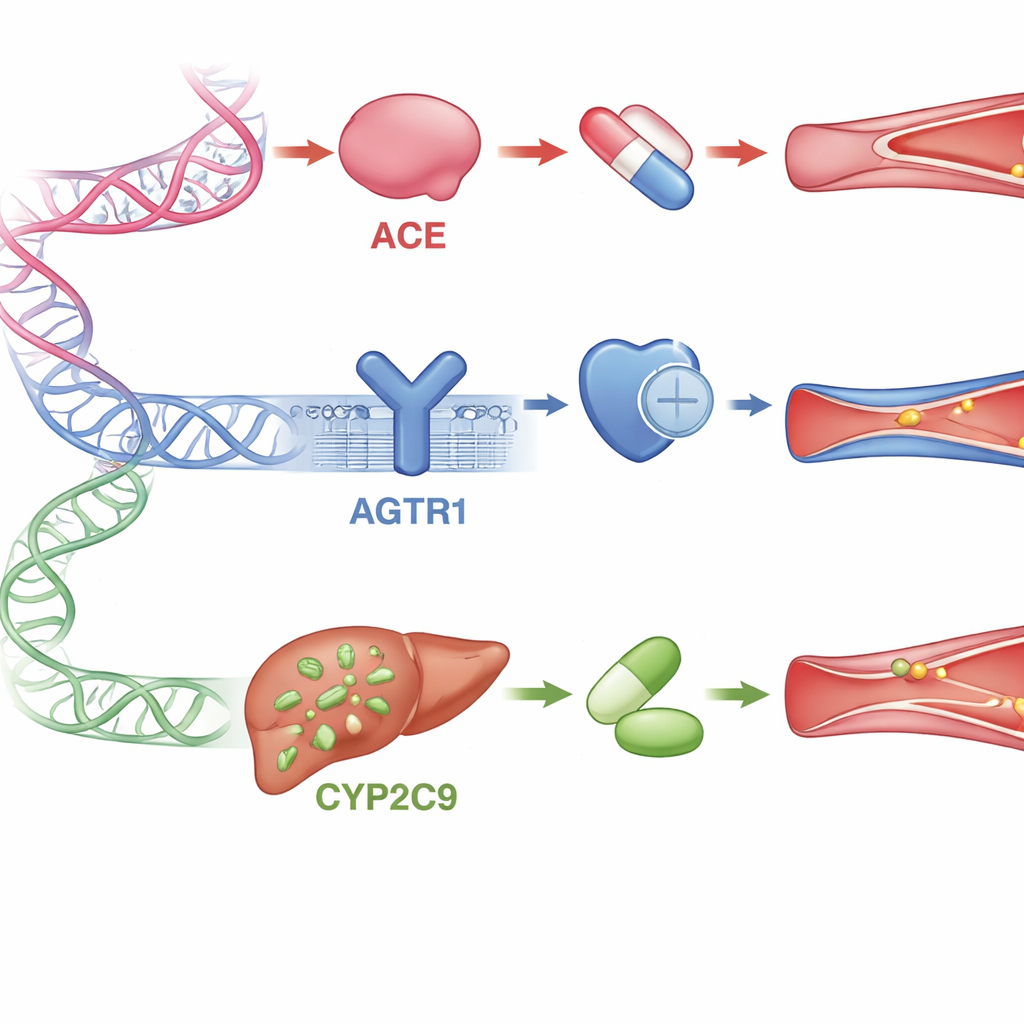
The review focuses on three important genes involved in this hormone system and in drug handling. The ACE gene controls production of the enzyme that creates the vessel-tightening hormone; certain small changes in this gene have been linked to weaker responses to ACE inhibitor drugs in many non-African populations. The AGTR1 gene encodes the main receptor that ARB drugs block; some variants appear to make the receptor behave differently or change how well the drugs attach to it, although studies in Africans and in other groups have sometimes found conflicting results. The CYP2C9 gene encodes a liver enzyme that breaks down or activates several ARB medicines. People with particular versions of this gene may process these drugs too slowly—raising the risk of side effects—or too quickly, leading to poor blood pressure control. For all three genes, African data are scarce, even though Africa has the greatest genetic diversity on the planet.
Why African Genetic Diversity Matters
Worldwide, research has shown that using genetic information to guide blood pressure treatment can improve control and reduce costs by avoiding trial-and-error prescribing. Yet two major obstacles limit these benefits in African settings. First, pharmacogenetic testing—the use of DNA tests to choose or adjust medicines—is rarely available in routine care, largely due to cost, limited laboratory capacity, and a shortage of trained staff. Second, most existing genetic studies and databases are based on European and Asian populations. Only a handful of African communities are represented in large global projects, leaving many variants undiscovered or poorly understood. As a result, treatment guidelines and “actionable” gene–drug recommendations may not fit African patients well, and relying on data from African Americans or other mixed-ancestry groups can be misleading.
Steps Toward More Personal Treatment
The authors argue that Africa needs both better implementation and better discovery. On the practical side, a stepwise approach could begin with a small set of well-proven gene–drug pairs and low-cost tests, paired with simple decision tools for clinicians. At the same time, stronger investment in local research, biobanks, and training would help map how often important variants in ACE, AGTR1, CYP2C9, and other genes occur across the continent’s many populations. Together, these efforts could move hypertension care away from one-size-fits-all prescribing toward approaches that use each person’s genetic and clinical information to choose safer, more effective medicines. For patients, that would mean a better chance of living longer, healthier lives with well-controlled blood pressure.
Citation: Gomera, R.T., van Hougenhouck-Tulleken, W., Brand, S.J. et al. Hypertension pharmacogenetics and limitations in Africa – a focus on the ACE, AGTR1 and CYP2C9 genes. J Hum Hypertens 40, 139–146 (2026). https://doi.org/10.1038/s41371-026-01121-0
Keywords: hypertension, pharmacogenetics, African populations, ACE and ARB drugs, precision medicine