Clear Sky Science · en
Expert consensus on orthodontic-associated alveolar ridge augmentation for adult patients
Stronger foundations for adult braces
Many adults hope that orthodontic treatment can finally give them a comfortable bite and confident smile. But unlike teenagers, adults often have thinner jawbone around their teeth, old areas of bone loss where teeth are missing, or wear and tear from past gum disease. This expert consensus article explains a way to safely "reinforce the foundations" around teeth with bone-building procedures so that orthodontic tooth movement is safer, more predictable, and less likely to damage the gums and supporting bone.
Why bone support matters for tooth straightening
In healthy mouths, teeth sit inside a sleeve of bone called the alveolar ridge, wrapped in gum tissue. In many adults, this bony sleeve is weakened or partly missing in spots, creating what dentists call bone defects. Moving teeth through these thin or missing areas can trigger problems such as receding gums, loosening teeth, loss of bone, or even damage to the tooth nerve. The authors emphasize that adult jawbones are less adaptable than those of adolescents, so the “hard limits” of the bone matter more when planning orthodontic treatment. Modern 3D X‑ray scans have revealed that these hidden weak spots are common, especially in patients with long‑standing tooth loss or pronounced jaw and bite discrepancies.
Rebuilding the ridge to guide safe movement
To tackle this problem, specialists increasingly pair orthodontics with alveolar ridge augmentation – adding bone graft material under a protective membrane to thicken and reshape the ridge. In this article, the term "orthodontic‑associated alveolar ridge augmentation" (OARA) is used for procedures whose main goal is to make tooth movement safer; any speed‑up of treatment is considered a bonus. The expert panel describes when this approach is most useful: when closing spaces where teeth have been missing for a long time, when clear bone defects already exist before treatment, and when planned tooth movement would otherwise push roots outside the natural bony envelope. Carefully chosen adult patients with good gum health and general health stand to benefit most.
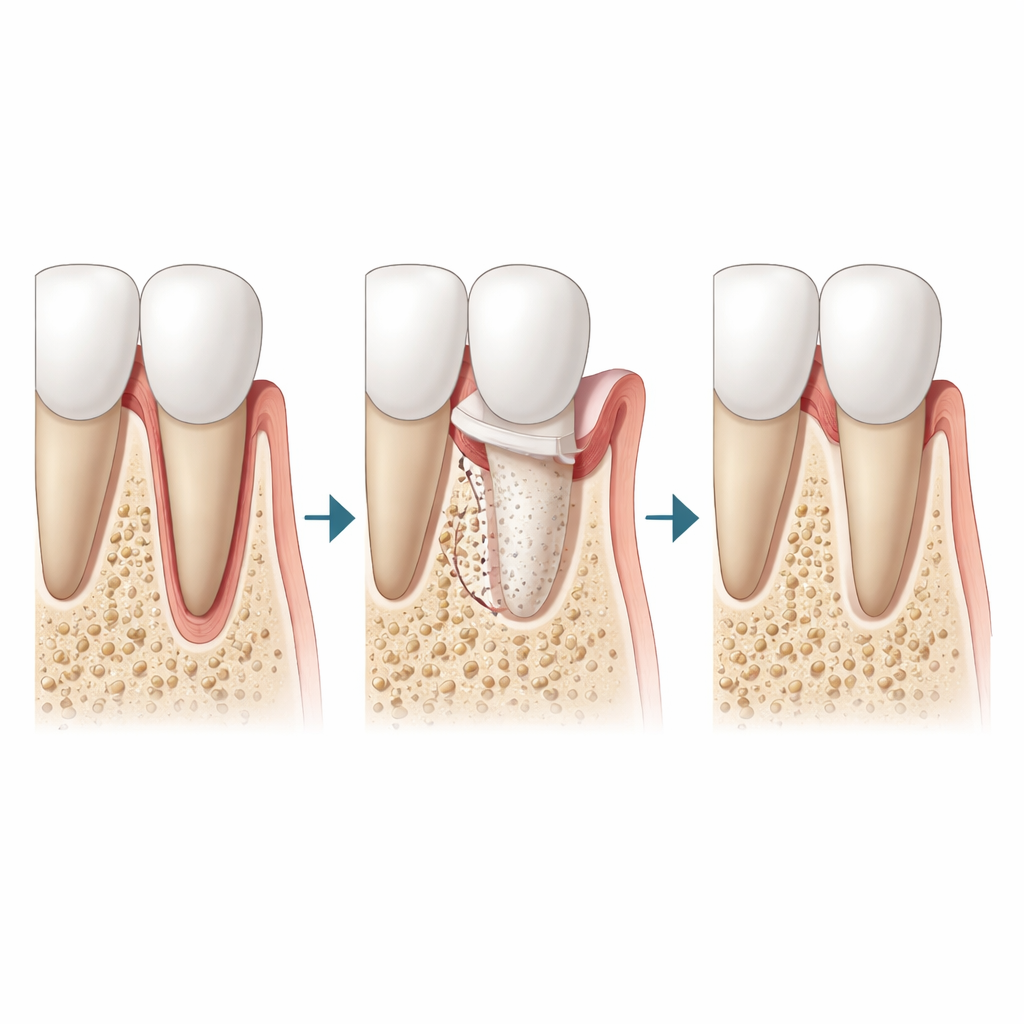
Materials and methods behind the bone build
OARA uses a mix of surgical finesse and biomaterials. Surgeons lightly score the outer bone around target teeth to stimulate local remodeling, then pack in graft particles that act as a scaffold for new bone. These grafts can come from a patient’s own body, human donors, animals such as cattle, or lab‑made ceramics and calcium‑based granules. Animal‑derived bovine grafts combined with a thin collagen membrane are currently the workhorse choice in practice, providing stability and a friendly surface for bone‑forming cells while allowing teeth to move through the area after healing begins. Synthetic materials and biological boosters like growth factors or platelet concentrates can be added to coax more vigorous bone formation, although the evidence base for some of these combinations is still developing.
When to operate and how to coordinate with braces
Timing turns out to be crucial. If bone augmentation is done too early, grafts may not receive enough mechanical stimulation from moving teeth to mature well; if done too late, teeth may already have strayed into danger zones. The consensus recommends tailoring timing to the treatment goal: in extraction cases, augmentation is typically done after initial alignment, just before pulling front teeth backward; in non‑extraction cases with planned outward movement of teeth, augmentation is done before significant movement begins. Light orthodontic forces are generally started about two weeks after surgery, when the gums have healed, and adjusted more often during a several‑month window when the bone is especially responsive.
Real‑world uses and current limitations
The panel illustrates OARA in three common adult scenarios: moving lower front teeth in severe underbites, retracting protruding front teeth after extractions, and closing long‑standing gaps where molars or other teeth are missing. In each, strengthening the ridge helps prevent gum recession and root exposure while expanding what is safely possible with orthodontics alone. Still, the experts caution that present techniques have limits. Thickening the crest of the ridge near the gumline is harder than adding bone near the root tips, graft exposure can occur if soft tissue closure is imperfect, and these methods cannot replace jaw surgery for very severe skeletal imbalances. Good gum care and regular monitoring remain essential during and after treatment.
Looking ahead for safer adult orthodontics
Overall, the consensus concludes that pairing bone augmentation with orthodontics can make adult treatment safer, extend the range of correctable problems, and support better long‑term stability, provided it is reserved for carefully selected cases and performed by experienced teams. However, many recommendations still rest on modest‑sized studies and clinical experience rather than large, long‑term trials. Future research on improved graft materials, more predictable bone gain near the gumline, and standardized protocols will help refine when and how to use OARA so that more adults can straighten their teeth without compromising the health of the bone and gums that hold them.
Citation: Guo, R., Li, X., Hou, J. et al. Expert consensus on orthodontic-associated alveolar ridge augmentation for adult patients. Int J Oral Sci 18, 29 (2026). https://doi.org/10.1038/s41368-026-00430-x
Keywords: adult orthodontics, bone grafting, alveolar ridge, gum health, tooth movement