Clear Sky Science · en
Associations between anthropometric and body composition indices with subclinical arterial damage in chronic inflammatory diseases
Why body size and artery health matter
Doctors often use simple body measurements—like weight, body mass index (BMI), and waist size—to estimate a person’s risk of heart disease and stroke. These easy tape‑measure tools work fairly well in the general population. But many people live with long‑lasting inflammatory conditions, such as rheumatoid arthritis or lupus, which already raise their heart risk through ongoing inflammation. This study asked a crucial question for these patients: can the same familiar body measurements still warn us about early artery damage, or does chronic inflammation change the rules?
Taking a closer look at the body and the arteries
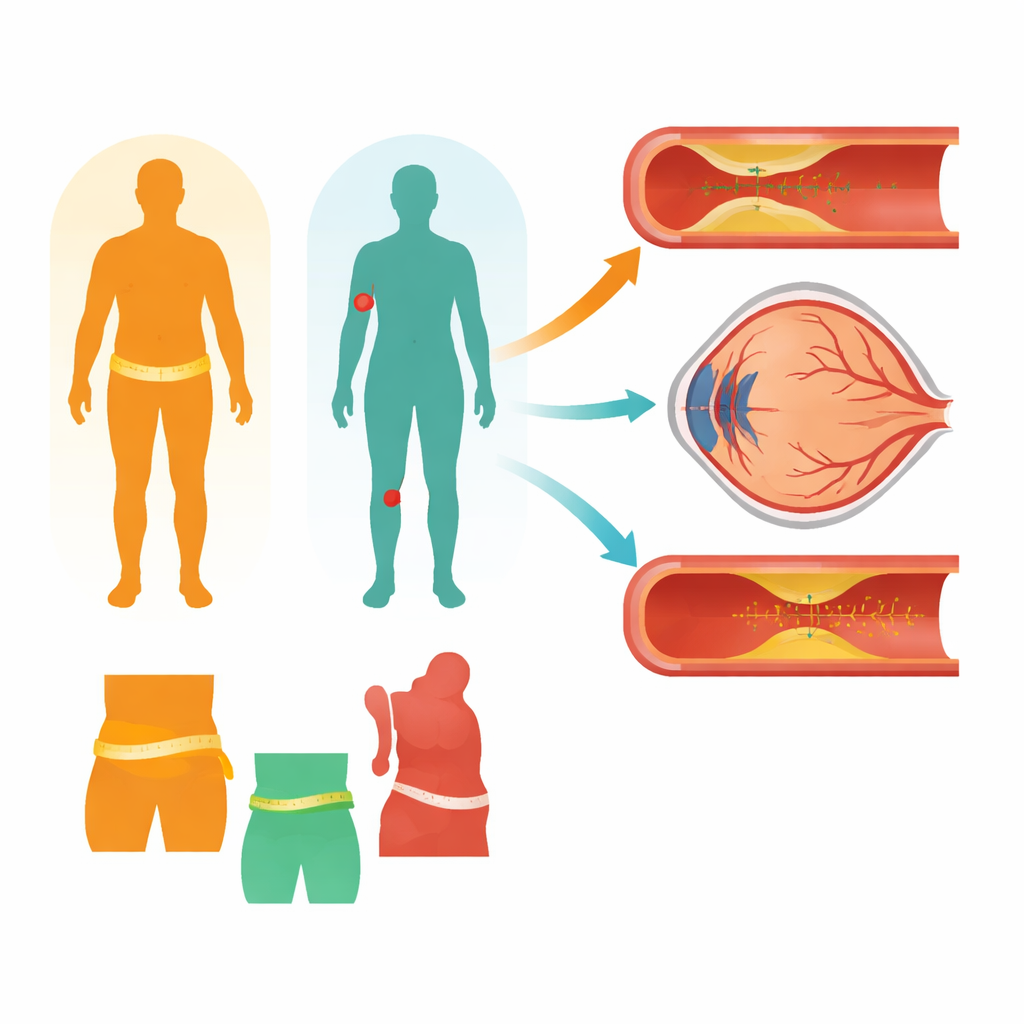
The researchers examined 755 adults in Greece. About two‑thirds had common cardiovascular risk factors—such as high blood pressure, high cholesterol, or smoking—but no chronic inflammatory disease. The remaining participants had chronic inflammatory diseases, including rheumatoid arthritis, systemic lupus erythematosus, systemic sclerosis, and spondylarthropathies, yet none had known heart or major blood vessel disease. Everyone underwent careful body measurements: weight, BMI, waist and hip circumferences, waist‑to‑height and waist‑to‑hip ratios, mid‑upper arm circumference, and estimated body fat percentage using a bioimpedance scale.
Hidden signs of artery wear and tear
To detect “silent” artery damage before symptoms appear, the team used three non‑invasive tests. Ultrasound scans measured the thickness of the inner wall of the neck (carotid) arteries, a marker of early build‑up and stiffening. A pulse wave test along the main artery from the heart to the leg gauged how stiff the aorta was. Finally, photographs of the back of the eye captured the tiny blood vessels in the retina; their width patterns are known to reflect long‑term blood pressure and cardiovascular risk. Together, these tests offered a window into both large and small blood vessels throughout the body.
What body size means without chronic inflammation
Among people who did not have chronic inflammatory disease but did have other cardiovascular risk factors, the usual story held true. Higher body weight, larger waistlines, greater BMI, and higher body fat were consistently linked with thicker carotid artery walls. These same measures were also related to less favorable patterns in the eye’s small blood vessels—narrower arterioles and wider venules—changes associated with a greater chance of future heart problems. In other words, for this group, simple body measurements still worked as reliable warning signs of early artery damage.
When inflammation rewrites the body’s signals
The pattern changed strikingly in patients with chronic inflammatory diseases. In this group, the typical body indices—weight, BMI, waist‑to‑hip ratio, and waist‑to‑height ratio—were no longer clearly related to early artery injury. Only three measures stood out: body fat percentage, mid‑upper arm circumference, and waist circumference showed modest links to thicker carotid artery walls. None of the body measurements were tied to changes in the small retinal vessels, and none were meaningfully associated with stiffness of the aorta in either group. Patients with chronic inflammatory disease generally had lower weight and BMI but slightly higher body fat and smaller arm circumference, reflecting a shift from muscle toward fat mass—an altered body make‑up driven by inflammation, inactivity, and some treatments.
What this means for people living with inflammation
For people without chronic inflammatory disease, familiar measures such as BMI and waist size still give useful clues about early blood vessel damage and heart risk. But in those living with long‑term inflammatory illnesses, these simple tape‑measure tools tell only part of the story—and may even be misleading. Because inflammation can reduce muscle and reshape where fat is stored, classic indices may no longer track well with how much harm is happening inside the arteries, especially in the smallest vessels. The study suggests that doctors may need more refined ways to assess body composition and vessel health in chronic inflammatory diseases, focusing not just on “how big” someone is but on how much fat, how much muscle, and where that fat is located. Future research will be needed to find the most accurate markers so that cardiovascular risk can be detected and prevented earlier in this growing group of patients.
Citation: Kaloudi, P., Protogerou, A.D., Aissopou, E.K. et al. Associations between anthropometric and body composition indices with subclinical arterial damage in chronic inflammatory diseases. Int J Obes 50, 887–894 (2026). https://doi.org/10.1038/s41366-026-02019-0
Keywords: chronic inflammatory disease, body composition, subclinical arterial damage, cardiovascular risk, anthropometric indices